
(Please welcome Tim Vaughan to Health Rising’s team of bloggers as he digs deeper into issues raised in earlier blogs and outlines an intriguing theory about the nature of pain in fibromyalgia, chronic fatigue syndrome and other disorders.)

In allodynia the lightest touch can be painful
Touch the tip of your forefinger to the tip of your thumb so that you are almost making that sign for, “all’s well”. Now imagine that when the two tips touch, it hurts. A lot! Now, imagine that any light touch of your fingers produces the same results: typing, petting an animal, tapping the screen of your smart phone/tablet… the list can go on and on.
This is allodynia, a dysfunction of the sensation of touch which has long been associated with Chronic Regional Pain Syndrome, but is nowadays recognized in the medical community as a prominent feature of fibromyalgia, migraine and even chronic fatigue syndrome (ME/CFS). Almost 80% of FM patients tested positive for allodynia in one study.
A Wide Reach
Allodynia is not confined to the fingertips, it can occur anywhere on the body. It can make wearing clothing, or hugging a nightmare. Still trying to conceptualize the hypersensitivity associated with allodynia? Think of the last time you bruised your toes or fingers. They became inflamed and swelled. When you lightly touched them they hurt like hell. When your clothing brushed against that spot, it was almost unbearable! That’s allodynia.
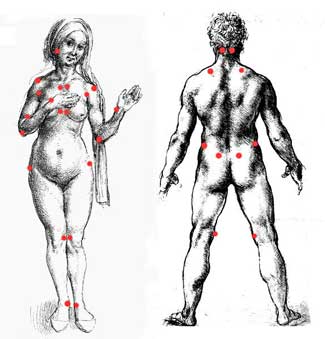
Are the tender points in FM in part tender because of reduced blood flows and ischemia?
If you have ever read about fibromyalgia, one of the primary concepts is the existence of “tender points”. My guess is that these tender points are just spots displaying the hypersensitivity of allodynia. Allodynia is a relatively new term in the medical field but several different types have been identified:
1. Mechanical/Tactile allodynia
- Static mechanical allodynia – pain in response to light touch/pressure
- Dynamic mechanical allodynia – pain in response to brushing
2. Thermal allodynia – pain from mild hot or cold temperature applied to the skin.
Mechanical allodynia is possibly the most persistent disabling symptom I experience. Often considered a nervous system phenomenom and labeled as nerve pain, some evidence suggests, it may be more due to muscular ischemia-reperfusion and autonomic system dysfunction than actual nerve injury.
I recently learned about ischemia-reperfusion injury when, after a stroke, my father was diagnosed as having Transient Ischemic Attacks (mini strokes). It was difficult for me to get my mind around this concept of ischemia-reperfusion injury until I read this explanation from Cort’s recent blog on exercise, muscle pain, and ischemia:
‘Ischemia’ occurs when blood flows to a tissue are low enough to reduce the level of oxygen and glucose needed for cellular energy production. The problem is actually not the ischemia per se but what comes after it; in what must be one of nature’s weirdest tricks, re-infusing tissues that have been deprived of oxygen with oxygen again can cause a serious problem called ‘reperfusion injury’.
It turns out that the absence of oxygen – which means the switching on of anaerobic metabolism and the production of toxic-by products – creates an environment posed for inflammation. Oxygen is a mild free radical and throwing it back into an oxygen deprived environment can result in an explosion of stronger free radicals such a nitric oxide, superoxide and finally peroxynitrite (e.g. Dr. Pall’s). Bizarrely, as that’s going on white blood cells may also bind to the endothelial cells lining the small blood capillaries, once again blocking the flow of the blood….Depriving your cells of oxygen is not something you want to do, even temporarily.
The Ischemia-Reperfusion Allodynia Connection
What does muscle-ischemia have to do with pain so severe that the lightest touch can cause extreme pain? Perhaps a lot…That explanation above sets the stage for a look at a 2008 paper on mechanical allodynia, “Cutaneous Tactile Allodynia Associated with Microvascular Dysfunction in Muscle”.

Reduced blood and oxygen flows to the muscles in ME/CFS/FM could set the stage for allodynia and other pain problems
Canadian researchers at McGill University investigated whether an ischemia-reperfusion (IR) injury produced allodynia in rats, and whether that allodynia was associated with micro-vascular dysfunction in muscles. First they induced allodynia symptoms in the hind foot of the rats, and then showed that micro-vascular dysfunction leads to persistent muscle ischemia and allodynia. Their statements ring similar to some in Cort’s “ischemia” blog:
…it is likely that allodynia depends on ischemia-reperfusion injury and resultant micro-vascular dysfunction, which may include arterial vasospasms and capillary slow flow/no-reflow. Arterial vasospasms occur due to a reduction in nitric oxide-induced vasodilatation and hyper-responsiveness of arterial smooth muscle cells to norepinephrine.
Capillary slow flow/no-reflow is the phenomenon that Cort mentioned in his “ischemia” blog where the capillary walls become clogged with platelets and white blood cells, thus blocking oxygen from reaching the muscle. Now the muscle has to deal with lack of oxygen and the inflammation cascade from reperfusion. As Cort mentioned, this sets up a great environment for the generation of pain.
Next, the McGill group measured lactate levels associated with the muscle ischemia and found evidence that increased lactate was associated with ischemia induced muscular allodynia in the rat’s hind paws. Cutaneous nerve abnormalities were not associated with the muscle ischemia, meaning this was not a dysfunction of the nerves per se, instead, it appeared to result from ischemia-reperfusion, vasospasms and the resulting lactate buildup.
“A Strong Reluctance to Exercise”

Muscle ischemia induced pain made rats ‘reluctant to exercise’. Is the same issue occurring in fibromyalgia and chronic fatigue syndrome?
They also found that these rats exhibited, “a strong reluctance to exercise” presumably because exercise made their allodynia and muscle pain worse. They suggested that muscle ischemia results in the generation of a higher basal (at rest) level of lactate in these rats contributing to pain and allodynia at rest.
After forcing these poor rats to exercise they found high levels of lactate and exercise-induced persistent pain and allodynia occurring days later. Maybe I should repeat that for emphasis…the rats experienced increased pain days after the exercise. That sure sounds a lot like a form of postexertional malaise to me.
Anybody else perplexed by the elevated pain and misery you experience the next day and the day after performing some sort of muscular exertion? Could these ‘allodynic’ rats experiencing the same thing people with ME/CFS are?
The Muscle -Central Sensitization Link
Then the McGill group turned to looking at the “central sensitization” of allodynia in these rats. They noted that other researchers could induce allodynia for several hours by injecting nerve pain-producing substances (capsaicin or carrageenan) into the skin
The McGill study suggests low blood flows to the muscles can induce long-lasting pain and allodynia
Injecting these substances into rat muscles produced a very different story; this time the central sensitization and allodynia lasted much longer, up two weeks. Something about muscle induced as opposed to skin induced allodynia causes a much longer period of ‘system reset’.
The McGill researchers believe the micro-vascular changes associated with ischemia constantly prime the phenomenon of “central sensitization of pain”, resulting in prolonged long-term central nervous system sensitization that shows up in allodynia, muscle dysfunction and way too much pain.
Anybody out there have tight, ropey, hard-feeling muscles that become fatigued and painful (with associated allodynia) way, way too easily?
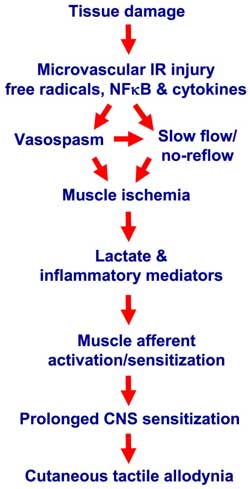
These authors take on the central sensitization (and the resulting pain) in fibromyalgia is different than most researchers who concentrate on the brain and changes in the brain from sensitization. The brain researchers have relied on brain imaging studies and measuring catecholamine (serotonin, dopamine, norepinephrine, etc.) changes in the brain’s chemistry. The McGill University’s researchers maintain changes in the micro-vascular structures of the muscles cause a cascade of events that constantly sensitize the muscles and the skin to pain, resulting in ever continuing central sensitization. As this diagram of theirs shows:
Figure 1. Laferriere, et al., “Schematic diagram indicating proposed mechanisms for initiation/maintenance of cutaneous tactile allodynia after IR injury”, figure 7, October 2008, Molecular Pain,4:49.
Considering the information in this McGill University study, an alternative clinical approach to try to alleviate allodynia might to focus on the autonomic system rather than relying on the commonly used approach of brain drugs (Cymbalta, Savella, Gabapentin, etc.).
What is causing this micro-vascular ischemia and reperfusion? One possibility is an autonomic system is in disarray resulting in too much constriction of the micro-vascular system resulting in ischemia and the resultant reperfusion damage. Do you have postural orthostatic tachycardia syndrome (POTS)? You have a dysfunctional autonomic system. You have allodynia? You might have a dysfunctional autonomic system as well. Do you have have muscle pain? You might have a dysfunctional autonomic system as well.
- Find ways to increase blood volume and perhaps avoid some ischemia in Enhancing Blood Volume in Chronic Fatigue Syndrome and Fibromyalgia



This was very informative and well written. I look forward to hearing more from Tim in the future.
Thanks, again, Cort, for all you do. I wish the English language had a better word to express how much I truly do thank you for keeping all of us so informed. Your work is invaluable.
Jeanie
Thanks Jeanie and thanks to Tim for jumping in and digging this information up. I had no idea allodynia or central sensitization could have anything to do with muscle ischemia. What a fascinating connnection that is..
I have long been interested in reperfusion injury and ME. The reason is its associated with both a rise in free arachidonic acid (which can be converted to inflammatory eicosanoids) and this arachidonic acid is associated with an oxidative stress burst from the mitochondria, but when I was investigating this 10 years ago or so the mechanism was not known.
It is also worth noting that stopping arachidonic acid from converting to eicosanoids usually prevents death by alcohol poisoning. Its the eicosanoids that typically kill someone who has consumed too much alcohol, inducing a massive inflammatory response. Alcohol causes arachidonic acid to be released from cell membranes, and once free it can convert to eicosanoids. Those with ME often cannot tolerate alcohol.
If Julia Newton’s work on muscle in CFS is right, then it would appear the muscle in CFS is acidic after exercise, but alkaline at rest. This kind of study needs to be done for fibromyalgia, Julia Newton took muscle biopsies and tested them. Isolating the muscle for testing taught her things that were not easy to show otherwise.
Alex.
Fascinating Alex – if I remember correctly, arachidonic acid or its equivalent is increased in ME/CFS? My alcohol intolerance goes up after I exercise; I assume that I’m whacking my system pretty hard with oxidative stress with exercise.
Fabulous article Cort.
P.S. I can personally account for, as well as what is reported by other patients, that Raynaud’s is very painful on rewarming, and that livedo reticularis , thought to have a sympathetic nervous system involvement, is alive and well in many FM patients. This study certainly brings these two elements together.
Such a great explanation of the study. Thanks again. And welcome Tim.
In healing and hope, Celeste
This article reminded me of an article I remembered reading recently on Regional Pain Syndrome, here’s the link:
http://www.rsds.org/pdfsall/Systemic-Complications-of-CRPS.pdf
Seems others are connecting this very thing. Reperfusion issues seems to be a big possibility and the connections to the autonomic nervous system – showing very likely.
I have been recently using grapefruit seed extract and having some pretty amazing results with it. I found an article of a study done with this to help in pancreatic reperfusion issues. Here is the link. Thinking if it helps the organs that much – maybe, it will help the muscles and skin with those type of issues too. Since I do have POTS and FMS along with EDS – this is a big concern for me because I have PEM and lots of pain from EDS and autonomic nervous system disorders. The results seem very significant and may be of help to others. I’m using 5 drops in water in the a.m. Would like to hear if it helps others too.
http://jpp.krakow.pl/journal/archive/12_04/pdf/811_12_04_article.pdf
There was another article saying that Alpha Lipoic Acid helps in liver reperfusion issues. This is also known to help with neuropathies. Makes you wonder if reperfusion is part of the issue with the neuropathies that we have with POTS too.
http://www.ncbi.nlm.nih.gov/pubmed/17259747
Great article. Looking forward to more thoughts and ideas.
Issie
You’ve got a trifecta! (POTS, FM and ED). Thanks for the suggestions..
Ha!Ha! Yeah, and you can add MCAS to that too. So what would you call that? Quadruple trouble! (Also issues with protozoa and co-infections.) Lot’s of stuff.
Just a quick note on the Grapefruit Seed Ext., I can’t believe how good I’m feeling with it. It’s been 3 weeks now and I’m well past the point of where things fizzle with me – where they will work for awhile and then stop. This is just getting better. I’m very encouraged with it. (It is a natural antibiotic, anti-viral, anti-bacterial, anti-parasitic and helps with inflammation. If it improves blood flow and helps with the immune system too —you are covering so many of the bases that may have to do with what all we have going on.)
Issie
Thanks for post!
I will just draw your attention to this paper “Neuroinflammation, Neuroautoimmunity,
and the Co-Morbidities of Complex Regional Pain Syndrome” http://www.rsds.org/pdfsall/JNIP-article-Cooper-Clark.pdf
“Complex Regional Pain Syndrome (CRPS) is associated with non-dermatomal patterns of pain, unusual
movement disorders, and somatovisceral dysfunctions. These symptoms are viewed by some neurologists and psychiatrists as being psychogenic in origin. Recent evidence, however, suggests that an autoimmune attack on selfantigens found in the peripheral and central nervous system may underlie a number of CRPS symptoms….
Recent discoveries have helped to elucidate possible mechanisms for the initiation and progression of CRPS. In general, neuroautoimmune responses are determined by how infiltrating leukocytes react to autoantibodies, which bind to autoantigens located on the surfaces of neuronal and glial cell targets (Fig. 1). For a substantial fraction of adult CRPS cases (Kohr et al. 2011), initiation of CRPS may lie in a breakdown of immunologic self-tolerance, and the development of autoantibodies to the β2AR and M2R neurotransmitter receptors.”
Please, do take your time to read the full arcticle, it is very interesting.
All the best :-))
Fabulous paper Helle
Neuroinflammation can explain a wide range of conditions previously described as ‘psychogenic’ or ‘medically unexplained’. They propose the following structural, functional and dynamic mechanisms :
Infiltration of autoantibodies into nervous tissues (functional
lesion)
– Infiltration of leukocytes into nervous tissues (structural/
functional lesion)
– Focal sites of cytokine imbalance (functional/dynamic
lesion)
– Remote neuroimmune activation of glia (structural/
functional lesion)
– Breakdown of blood brain barrier (structural lesion)
– Loss of inhibitory tone (functional lesion)
– Excessive loop gain in neural circuits (dynamic lesion)
– Thalamic neuroinflammation (structural/functional
lesion)
– Loss of sensory gating (functional lesion)
– Synaptic conversion (functional lesion)
– Thalamocortical dysrhythmias (dynamic lesion)
– Distortion of a somatotopic map (structural/functional
lesion)
– Altered connectivity within the brain (dynamic/functional
lesion)
Wow this report makes a lot of sense especially when a flare up causes sooooo much pain that no one can come near you. I also experience Reynards although my skin reacts to any change in temperature hot or cold can be very uncomfortable.
I am really happy that have found this web site as often I feel I’m alone in the way my pain and fatigue affects me. THANKYOU
An interesting article..one I will follow up on in terms of research. I developed very severe body-wide allodynia for the first time 19 months ago, 41 years into my ME. I had developed an ‘oddly presenting’ cat allergen out of the blue 7 months previously (the cat was eventually re homed). The odd reaction was not respiratory in any way…my skin would itch and prickle and sting, more at some times than others. I could still wear normal clothing (ok not totally normal..I’ve had sensitive skin from year ‘dot’ but sensibly chosen clothing never caused me any pain or irritation). Then suddenly, almost overnight, the pain changed to what I discovered was this dreadful, hideous, life changing thing called ‘allodynia’. I won’t go into great details to describe it other than to say I contemplated taking my life until I eventually had the roughest edges of it reduced by pregabalin, but as everyone with this condition probably knows, and to paraphrase The Verve, ‘the drugs don’t work’..well not well enough anyway. I sit here typing this feeling as though someone has poured caustic soda all over me..I also sit here draped in silk satin, it being one of the very few fabrics not to make the pain any worse than it is.
My ponderings thus far (in addition to the presumption that maybe some sort of dorsal root ganglionitis is at the source of this condition) is that allergy may play a part too. Not least because the genesis of my pain seemed to occur in tandem with a peculiar allergic response which I’d never had before, plus it’s clear certain foodstuffs trigger worse pain, and of course Health Rising has also reported on the findings which link increased clusters of mast cells under the skin of people with allodynia. Therefore this report presents a whole new way of looking at this condition. Given that I haven’t experienced bad pain in the whole of my 43 years of ME until this recent occurrence, and still get little muscle pain (unless I’ve ‘overdone’ it..which frankly requires little effort) does this theory as detailed above tie into my history and presentation I wonder?
I’d certainly love to hear any feedback from anyone who may be able to enlighten me. In all these years this is unequivocally the worst thing which has ever happened to me…if I can gain greater understanding to do things (or equally avoid things) which could have a beneficial bearing on this pain I would be eternally grateful.
Amazing Floydguy – I really feel for you and hope you can find some way to get out of this…My girlfriend has allodynia on her right leg; it’s probably her worst symptom. I know someone else with major skin hypersensitivity..
An interesting publication will be out soon on dorsal root ganglia, pain and FM…It may provide something of interest to you. I’m definitely looking into that area…Among other things I think the linkups are fascinating..
Its amazing how the body can switch to a new state so quickly…Maybe it can switch back at some point.
Good luck!
Thanks Cort..I presume this reply was aimed at me, not ‘Floydguy’..or maybe both of us?…but I will await the publication you mention with interest..I just hope it may include ideas about better treatment, as what exists presently is far from acceptable.
My neurologist says these things can ‘just go’ ..I very much hope this will..sooner rather than later. It hideous 🙁
thank you for this amazing article Cort! I sent it to all my govt contacts. so informative!
I’m very glad to see that someone has finally taken up this subject. I myself have believed for many years that allodynia is caused by trigger points (knots in the muscles) which are tiny highly electrified areas in the muscle that interfere with the microcirculation. The severity of trigger points increases over time and they spread like the domino effect. When severe they can spread to tendons, ligaments, subcutaneous tissue and the skin, resulting in pain in all these areas. I myself suffered quite severe allodynia more than 10 years ago but once I started treating the trigger points and eliminating as many perpetuating factors as I could, my allodynia all but disappeared. I thankfully got my sex life back! I still have trigger points and believe that with fibromyalgia, one can never be completely rid of them unless something can be done about the changes in the brain and neurotransmitters that are perpetuating them. I keep my trigger points pretty much under control by addressing as many of the perpetuating factors as possible and deal promptly and manually with any that become painful. As for allodynia, I still have a few slightly sensitive spots on the skin over my worst trigger point areas and if I let things get out of control, my overall allodynia may re-occur mildly during the flare that eventuates.
Interesting about the arachidonic acid and the eicosanoids, Alex, because one of the things that helped control the trigger points for me was the Zone diet . The author, Barry Sears, a biochemist, believes that his diet keeps the eicosanoids in balance (promotes good ones and helps eliminate the bad ones by reducing arachidonic acid). Other perpetuating factors I address by using bio-identical hormones (pregnenolone) and striving to keep my body pH neutral (I do this by using a balance of diet and physical activity but the diet needs to address one’s own metabolic type by using foods that change your pH in the way you wish.) I don’t take any prescription medication.
Excellent article Tim.
You’re spot on that the prevailing recent model of fibromyalgia has been based on the loss of central, top down inhibitory mechanisms that results in the ‘perception’ of widespread pain.
Peripheral ischemia and recent independent findings that fibro patients have peripheral neuropathies suggests that that central sensitivity may be the result of ongoing peripheral pain rather than the cause.
Given that ischemia is neurotoxic via a neuroinflammatory cascade, its plausible that ischemia could result in localised neuropathies. Both of which would feed back to enhance ‘central sensitivity’.
BTW – as I understand it the classic tender points are being gradually phased out of fibro case definitions. It has been suggested that these points are also ‘tender’ in healthy individuals and the enhanced pain in fibro just make them more so.
The involvement of autonomic dysfunction in micro-vascular constriction is also very plausible as the ANS seems to figure more and more in recent fibromyalgia and ME/CFS research.
Oh – and welcome 🙂
To all,
Thanks for the nice words and interesting comments. One question that keeps on wandering around my mind is how does one “fix” the autonomic system?
When I read the McGill University research article I noted that when the rats exhibited a “reluctance to exercise”, no one blamed it on psychological problems or lack of initiative. Too bad those rats didn’t have some medical doctors to advise them to go get some cognitive behavior therapy.
timv
So many of the things I read make me continue to wonder why Les Simpson’s work on the role of non-deformable erythrocytes continues to be completely absent from these discussions. It is such a simple concept, and verifiable just by looking at micrographs of immediately fixed red blood cells. The function of the red blood cells is to provide oxygen and remove lactates from all the cells in our body. The red blood cells are very sensitive to changes in their environment, and respond with changes in their shape. Most red blood cells are biconcave discocytes – perfectly round, with a dimple in both sides. This shape is very ‘deformable’, easily curling up to pass through the tiny capillaries (the microcirculation) which are narrower than they are, to perform their function for the cells the capillaries serve. When the red cell population starts having a high proportion of non-deformable shapes – the irregular ones that can’t curl up so easily – then the cells served by the smallest capillaries start suffering from oxygen deficiency and a build-up of lactates. The tissues in the body most sensitive to this oxygen deficiency and build-up of lactates are the muscles, the cognitive areas of the brain, and the endocrine system. This provides a simple and clearcut explanation for the failure of the aerobic muscle metabolism and the early shift to use of the anaerobic system after only slight exertion in people who have ME//FM. It also provides an explanation for our cognitive problems and the dysregulation of our endocrine system, and, reading the above, seems also to provide a possible explanation for the oxygen deprivation in the extremities which, it appears, is a significant cause of pain.
Occam’s razor, the principle that the simplest explanation should be given the most weight, and the concept of elegance in scientific research strongly suggest that these factors, the information provided by the field of hemorheology should be given a priority in our thinking about ME. When I read articles such as the above, and articles about immune system dysfunction, and the importance of inflammatory processes, it seems to me, again and again, that many apparent puzzles could be resolved if the information above were taken into account, as part of the whole complex set of systems involved in the pathophysiology of ME/FM
During the early 2000’s, Les travelled in the US, Canada, the UK, as well as in Australia, and in his own country, New Zealand, visiting ME support groups and ME patients who were housebound, taking blood samples for analysis, as well as providing a sympathetic and supportive presence in the ME community. His work has been corroborated when, for example, he has been sent blind samples to analyse, and he has observed changes in the red blood cell population which correlate with when patients are in remission and when having a crash – in remission, the red cell population reverts to normal proportions of biconcave discocytes.
His work has been brushed aside – for example, by small studies in which his protocol – the cells must be immediately fixed before being micrographed, in order to observe the shape changes- has not been followed. I don’t understand the thinking of researchers who prefer attempting to discredit the work of others, when incorporating it could be so valuable in actually helping solve the problems of ME/FM.
Insofar as the blood flow problems, which are recognised in the works quoted above, are caused by a high proportion of non-deformable discocytes in the red blood cell population, the good news is that there are several easily obtainable things which can improve this situation. Les suggests 6 g per day of fish oil (the higher dose than usually recommended is necessary to have any effect), or 4 g per day of genuine Evening Primrose Oil (again, this was discounted by a piece of research – but analysis of commonly used ‘EPO’ indicated that of 11 products sold as EPO, only 3 were genuine), or pentoxyfilline, or Vitamin B 12 as hydroxocobalamin (most B12 is cyanocobalamin). Following these suggestions has helped many ME sufferers.
I would strongly suggest that patients try out one or another of these products for six weeks, until they find one that works for them. Les has found that each of them can help a significant percentage of people who have ME – there are unanswered questions about why some don’t work for some people. But the level of desperation expressed in these comments does make me wish that more people had this information, therefore access to the possibility of some improvement in their symptoms by trying out these suggestions.
And I really do wish that researchers would take these observations into account in the process of constructing theoretical explanations – it seems to me that they do provide a simple, elegant and verifiable contribution towards understanding all the processes which contribute to this terrible illness.
Nancy,
Comments are interesting and appreciated. Besides your books on the subject, are there other sources that people can access to find out more details about this protocol? I personally have tried 6g of high-quality fish oil, etc. but I have never tried or heard of pentoxyfilline…. That prescription drug sounds like something I may follow up on. What causes the red blood cells to not be able to deform?
Interesting!
Some of us are addressing problems with Methylation Pathway genetic mutations and one of the things addressed with this is problems with Methyl B12. This is one thing that I’ve recently added to my mix.
I’ve not heard or read this information before. Thanks for posting it.
My doctor (Dr. Stephen Fry) feels that there may be issues with blood flow due to colonies of biofilm encased protozoa, bacteria and virus. He feels that these biofilms adhere to the walls of blood vessels and cause issues with blood flow and vein function. The biofilms becomes a hard – plaque like substance (think – tarter on your teeth) and would interfere with proper vein functioning in regards to dilation and/or constricting. My addressing my immune system and therefore breaking down this biofilm and causing the immune system to recognize these pathogens – seems to be making a huge difference with me.
Issie
I think i have this syndrome, have been to several doctors neurologists and rhumitoid doctors it is very frustrating that there is not a blood test or a real answer if you have it. i have been dealing with this for 3 years!!! off to Jefferson Neurologist tomorrow for hopefully more answers!!!
Good luck Mozey!
Sorry I lost what used to be good communication skillskills. This theory workd with the frequent concurrence of migraines = vasospasm, vasospastic angina, and fibro. Please stay on this and follow it to the end