


Newton’s Apples
Apples and ME/CFS patients; Gravity to Issac Newton, the ANS to Julia Newton
Issac Newton formulated the theory of gravity by watching an apple fall to the ground; Dr. Julia Newton has formulated a different theory of ‘gravity’ in ME/CFS ; she believes what’s causing ME/CFS patients to have so much trouble walking and exercising is not so much gravity as a mucked-up autonomic nervous system.
Clark Ellis’s interview with Dr. Newton examining these factors recently appeared in different forms on Prohealth and Phoenix Rising. In this blog we’re going to look at some highlights of that interview and dig a bit deeper into Dr. Newton’s work.
First we’re going to look at the fascinating connection between a disorder called primary biliary cirrhosis, which on the face of it has absolutely nothing to do with ME/CFS, and this disorder.
Primary Biliary Cirrhosis – A Model for Chronic Fatigue Syndrome (ME/CFS)?
Dr. Newton worked on primary biliary cirrhosis (PBC) before she began to work on ME/CFS. PBC is an autoimmune disorder characterized by T-cell destruction of the bile ducts in the liver that, ultimately, in some patients requires a liver transplant. Most PBC patients display auto-antibodies to mitochondrial cells as well. Like other autoimmune disorders (and ME/CFS) women dominate the PBC rolls.

Strange Partners
It is important to point out at this stage that the muscle and cardiac abnormalities that we have seen in patients with ME/CFS are exactly the same as those that we have seen in patients with PBC. Dr .Julia Newton
With its severe liver issues PBC seems like a strange cousin to ME/CFS but it turns out that similarities abound. Causing enormous and unexplained fatigue PBC is one of the few diseases fatigue is being fairly rigorously studied (mostly by Dr. Newton :)). The fatigue in PBC is serious; while it’s not directly killing patients, increased frequency of fatigue in PBC is associated with increased mortality.
 Some of Newton’s PBC findings are startlingly similar to those in ME/CFS. Newton’s finding that orthostatic intolerance is associated with cognitive issues in PBC suggested blood flows to the brain could be, as with ME/CFS, key factors in PBC. The activity of the ‘rest and digest’ system (parasympathetic nervous system) in both PBC and ME/CFS appears to be turned down, while the activity of the ‘fight or flight’ system (sympathetic nervous system) appears to ramped up.
Some of Newton’s PBC findings are startlingly similar to those in ME/CFS. Newton’s finding that orthostatic intolerance is associated with cognitive issues in PBC suggested blood flows to the brain could be, as with ME/CFS, key factors in PBC. The activity of the ‘rest and digest’ system (parasympathetic nervous system) in both PBC and ME/CFS appears to be turned down, while the activity of the ‘fight or flight’ system (sympathetic nervous system) appears to ramped up.
Increased rates of muscle acidosis and difficulty removing acid from the muscles are present in both disorders. As with ME/CFS PBC patients can have reduced cardiac output during standing. The stimulant, Modafinil can be effective in both ME/CFS and PBC, in increasing energy and reducing fatigue.
The fatigue in PBC also appears to be linked to impaired ‘central activation’ which refers to the ability of the brain to activate the muscles. Several studies (in the distant past), including one co-authored by Dr. Bleijenberg, of all people), suggested reduced muscle activation is present in chronic fatigue syndrome but research has lapsed in that area. The sequential activation of our muscles during exercise lifts the burden from any one muscle and helps reduce fatigue. The idea of impaired central activation of the muscles seems like a no-brainer in a disorder like chronic fatigue syndrome, and studies did suggest it might be present, but research in the area has lapsed.
Rituximab, Primary Billiary Cirrhosis and ME/CFS
I am optimistic that the results of the PBC study might apply to the ME/CFS too. Dr. Newton talking on the Rituximab trial in PBC
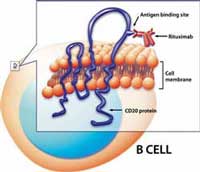
Dr. Newton believes the Rituximab findings in the PBC trial may hold true for ME/CFS as well.
Now Dr. Newton is testing Rituximab in PBC in an attempt to knock down the autoimmune process that’s whacking the liver bile duct cells in that disease. This isn’t the first attempt to use an immune suppressive drugs in PBC. A review of PBC methotrexate trials suggested that immune modulator did not reduce fatigue, mortality or rate of liver transplantation but it did improve several measures including immune one. (Methotrexate is commonly used with Rituximab)
All this has been a prelude to that fact that Dr. Newton has begun a Rituximab trial in primary biliary cirrhosis. An earlier study found Rituximab improved lab results in that disorder but did not improve fatigue but Dr. Newton clearly thinks her study will get different results. Ellis asked her if she thought the trial, if successful, might apply to ME/CFS – and she did.
“If we do see any changes in fatigue we may well gain information that will help us understand the mechanism by which that improvement occurs. It is important to point out at this stage that the muscle and cardiac abnormalities that we have seen in patients with ME/CFS are exactly the same as those that we have seen in patients with PBC and we have published these studies too which is one of the reasons I am optimistic that the results of the PBC study might apply to the ME/CFS too.”
Those Acid Accumulators
Some ME/CFS patients are accumulating large amounts of lactic acid in their muscles during ‘exercise’. Lactic acid has been a pretty tricky topic in ME/CFS. A early study found evidence for it but followup studies did not. Now Newton is finding enough of it to conclude it’s a major issue and has gone so far as to biopsy muscles, throw them into test tubes and then make them exercise, in order to figure out why. She’s finding the same acid accumulations in the muscles in the lab as she does with patients and she believes it’s possible to identify where the problem is, and….the biggie…. reverse the process, possibly with already available drugs.

Is muscle acidosis keeping ME/CFS patients muscles from looking like this?
What drugs might she be looking at? Unfortunately we didn’t get that nugget but we got a hint when Ellis asked if the autonomic nervous system might play a role. It turns out it might, by turning off the acid transporters in muscle cells, by locking down blood flow to the muscles (and impairing acid removal), and that suggests she’s looking at drugs that affect ANS functioning.
“Interestingly acid accumulation in the muscle is controlled by receptors or transporters on the muscle cell wall and some of these transporters are regulated by the autonomic nervous system so that would be one way that it works. Another way could simply be that the acid that is released from muscle cells is washed away and therefore is dependent upon the vascular system to ensure run-off of acid as the muscles exercise. The autonomic nervous system regulates the caliber of the blood vessels around muscles and this could therefore influence the muscles’ ability to get rid of acid. “
In the Naked Scientist interview, Dr. Newton reported she had some ‘very exciting’ pilot data which suggests she can reverse the acid accumulations using various medications and stated that she was in a very optimistic place”.
- The ‘Wolf’ in ME/CFS: Newton on a System Stuck in Overdrive – from my earlier blog on Phoenix Rising (not attributed) – on Dr. Newton’s work.
The Heart
One of Newton’s small studies found reduced cardiac mass and diastolic volume. (Some issues were left unresolved in this study, however. Patients and controls were matched for age, gender and height/weight but not for activity. Smaller hearts have been associated with reduced activity levels. She did note that she’s asked about deconditioning a lot Interestingly, a small study of muscle fiber characteristics did not find a predominance of the muscle fibers associated with inactivity (even though the participants were probably inactive (!)). Another found deconditioning was not a perpetuating factor in ME/CFS. )

Dr. Newton is bringing the heart….after a long absence – is back in play in chronic fatigue syndrome
In the cardiac paper Dr. Newton suggested that graded exercise therapies and saline IV’s might be able to increase cardiac blood volume in ME/CFS. Several times Dr. Newton, without giving more particulars, has suggested increased exercise might help some patients.
The heart is definitely back in play in chronic fatigue syndrome. It’s been awhile… Working out of Dr. Natelson’s NIH funded CFS research center (anybody remember those?), Arnold Peckerman had strong run in the early 2000′s, publishing no less than six papers in 2003 on cardiovascular and autonomic nervous system issues in CFS and GWI. Peckerman’s work was discontinued with the ’regime change’ at the NIH’s CFS team and the breakup of the centers. After 2005 he never published again.
Cognitive Problems
When Ellis asked Dr. Newton about the connection between the autonomic nervous system and cognition and then the muscles Newton felt those issues were probably caused by a system wide problem, that the muscles play a key role and she noted that she’s looking at the mitochondria closely.
“Interestingly, when we look at the muscle, brain and hearts of those who have had all three of these investigations there is a relationship between the abnormalities that we have found suggesting that any problem is not just related to one organ but is generalized across a number of organs. Our muscle studies have now extended into taking muscle biopsies from people and growing the muscle cells and we have also recently been looking at mitochondria.”
Conclusions
” Our results suggest that CFS subjects may have been suffering from a pathological sympathetic activity…. that has lead to their autonomic effectors (heart and blood vessels) becoming resistant to …stimulation”
The ANS appears to be involved in myriad of issues in ME/CFS and fibromyalgia and Dr. Newton is right in the thick of that research. it appears to be involved in poor cognition and sleep, fatigue, problems standing, pain and possibly immune regulation in these disorders.
Newton’s research suggests, like a boy calling wolf one too many times, the problem may simply be due to the autonomic nervous system turning a deaf ear to the body. She suggests that a chronically over-active sympathetic nervous system is simply no longer being heard, e.g; it tells the heart to fill – and it doesn’t…it tells blood pressure to increase – and it doesn’t; it tells the blood vessels to narrow (to force blood to the muscles, etc.) and they don’t. It’s as if the internal wiring of an important body-wide system is burned out.
Your Donations Keep Health Rising….Rising!



Cort,
Maybe Ive missed reading it, but does anyone know how to regulate the ANS?
You want treatment too! 🙂
There are ways to regulate the ANS and I’m getting a blog together on them..I have a few more blogs on the ANS to get out and we try the treatment end. The ANS, interestingly enough, is one of the few system we can exert some control over by controlling our rate of breathing, how deeply we breath, by reducing stress etc. There are also drugs – beta blockers and others – that can effect ANS functioning…I imagine Dr. Newton is testing those now…
Some studies should be coming out pretty soon that look at some ANS effecting drugs in ME/CFS, I believe.
Some being the operative word. One can’t easily do it when they sleep and it takes focused concentration which most of us don’t have. I work really hard at my breathing but have not had any success “flipping the switch” so breathing returns to normal when I am not thinking about it. I suspect that it’s not that the ANS is just broken but something is preventing it from working the way that it should. In my case I would toss out being in chronic inflammatory state.
Good points Floydguy – I vividly remember reading the story of a guy with some sort of ANS dysfunction who used meditation to keep it under control and it did help but there were times when his body would just have its way – usually about 2 am. . I think he had some sort of seizures.
I agree that focused attention comes very hard for us in general; that’s my experience..and that makes doing this kind of stuff more difficult.
I should have said breathing returns to an abnormal normal. Lol.
lol @ “no brainer”; yeah, that resonates.
🙂
Cort,
Thank you for this. It gives me some ideas on how to carefully improve my physical activity without pay-back!
Suella
The ANS is the central problem for most people with CVS NOT ALL. It will be a subgroup. I think that the parasympathetic nervous system is ”defect”. This route goes by the nervus vagus and interact directly with the immunesystem by marcrofacen within the stomach by example. An active nervous system also put down the immune system and reactivate herpes viruses etc… I say this for 15 year now.
Gijs….It was interesting to hear Suzanne Vernon, I think it was, say that one of their projects had identified a autonomic subset and an immune subset. I think I would be more in the ANS subset.
Hi cort, very interesting. I hope Vernon will publish her data soon. It works both ways ANS and the immune system. When the ANS is in overdrive for many years the immune system will also get serious problems like autoimmunity, damaged cells etc… The ANS is damaged by high fever or it is a genetic problem. Maybe we will never know the real cause 🙂
Yes – its a big immune regulator and will shove the immune system to Th2 as I remember…Not many people realize that…It’s fascinating stuff, for sure. 🙂
Fabulous! Keep up this incredible work.