


ME is a painful condition. Phillida, who has had ME in the past, trained in various physical therapies such as massage and reflexology and took an MsC in Complementary Therapy at Westminster University in the UK as a way of using the respite care she was provided while caring for her daughter who was having a bout of severe ME at the time.

Some of the pain in ME is produced by local constrictions in muscles. There is something you can do about them…
At the December 2013 meeting of the Wellington support group Phillida explained how two of these massage techniques, trigger point therapy and myofascial therapy, can be useful in relieving some ME pain.
Some parts of these therapies can be self-applied; for others you will need a friend or a trained therapist to help you. Crucially, these are gentle techniques which will not hurt you or make you worse, and they may be very useful. They are not cures, but they may help lighten the load of some symptoms.
The wonderful Jackie Stiencamp, of Christchurch, wrote Overload, published in the 1980s by ME sufferer Christine Cole Cately. It was one of the first books to clearly identify ME. Her approach to recovery was to unload as many of the stressors as possible. I found that approach very useful.
The therapies described here fit well into that model. If you are unable to access suitable practitioners you may find Bowen or Qigong useful as both use similar gentle techniques that are applicable to the fascia.
Trigger Point Therapy
(A slightly more complex version of trigger point therapy is called neuro-muscular therapy).
Trigger points are tender spots which can develop in any muscle that is inactive or under
As often occurs, trigger points lying in multiple points in the muscles
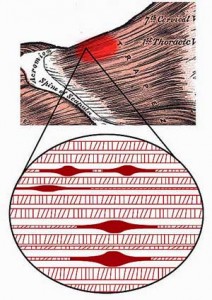
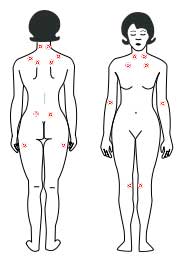
prolonged tension. There are characteristic patterns where these points develop. There is, for instance, about an 80% overlap between trigger points and the Ar-Chi points in acupuncture. Fibromyalgia has been defined as tenderness in a majority of 18 pairs of tender points found in symmetric locations around the body. Common locations for trigger points are the neck or shoulder, but it is important to note that they can develop in any muscle, including in your internal muscles.
Identifying trigger points:
- Running your finger along a muscle fiber you may feel a tight knot, possibly as big as a pea, but possibly more like a ‘taut guitar string’, depending on the size of the muscle fibers affected.
- Pressing on the spot will feel sore and produce a familiar pattern of pain.
- This ‘referred pain’ may radiate from that spot or may be distant from it.
- The pain may ‘sensitize’ your nerves creating horrible pain such as headaches, or it may make you feel nauseated or over-sensitive to light or other sensory stimulation.
The aim of therapy is to release these knots by restoring blood flow through the knot and allow the muscle to regain its ‘normal’ resting length. This will release both the muscle pain and the associated nerve pain.
The Theory: How Trigger Points Develop
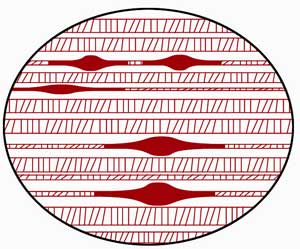
Muscles are designed to move. To facilitate movement each muscle fibre has rows of little evenly-spaced cells that are like air bags which change shape as the muscle contracts and elongates. These are called sarcomeres.
These sarcomeres bunch up at the center of contracted muscles and stretch out toward the ends of the muscles (which are called insertion points).
The same trigger point complex associated with the muscles it occurs in
Trigger points develop when these bunched up cells do not release and return to their normal resting length and uniform arrangement along the muscle fiber. The pain is likely to be worse towards the center of the muscle, but the stretched-out ends and insertion points may be sore too.
As the muscle works it gets nutrients and oxygen from the blood and uses the blood to carry away waste products. When healthy people do unusual amounts of exercise they create waste products more quickly than can be carried away and will feel stiff and sore. If they do gentle exercise the next day or have a massage or a hot bath to stimulate the blood flow, the stiffness will dissipate.
With ME/CFS, however, a well-established oxygen deficit and often reduced blood volume and blood flow can prevent the waste byproducts of contracted, stressed muscles from being carried away.
This waste removal problem is greatly enhanced by the bunching up of the sarcomeres which further restricts blood flow and the removal of metabolic wastes. The sarcomeres tend to bunch up most around the middle or fattest part of the muscle, which just happens to be where the nerve which controls the movement of the muscle usually enters and leaves the muscle.
As the waste products build up they restrict the oxygen supply further. This creates bunched-up ‘knots’ of tissue which overstimulate the nerves, leading to ‘neural sensitization’ and dramatically increased pain.
The pain may be further increased when it leads to ‘breath holding’ or a shallow up-tight breathing pattern. You cannot get enough oxygen with your shoulders hunched up against pain, plus knots may well form in the muscles you use for breathing.
Breath re-education can be a helpful adjunct to this therapy.
Therapy
You cannot just relax these knots; they need to have the blood supply restored for the muscle to relax and resume its normal length. This can be done by mechanical manipulation, but although you probably try and ease the feeling by rubbing along or across the muscle, this is unlikely to be very effective.
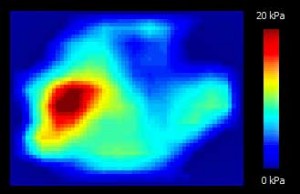
An image showing increased heat (inflammation) around the trigger point.
The best way is to use A PRESSURE AND RELEASE ACTION that will pump the blood through the knot of the tender point. There are a number of therapies which do some version of this.
‘Point holding’ is one, acupressure is another, and so is an acupuncture technique called ‘superficial dry needling’. Some find saline injections into the tender points to be effective. These techniques have to be spot-on accurate in location, however, in order to be effective. I find them generally less effective than the method described below:
- Identify the tender point. Run a finger along the length of the muscle and find the sore spot.
- Press on it, possibly at a slight angle. As you press on it you will feel a kind of nice/nasty pain with a familiar pattern of referred pain. (A really experienced therapist will be able to identify the tender spot from your description of the referred pain pattern, but the books which show common pain pattern maps of the body are also useful.)
- Press into the knot to a count of 8.
- Release for a count of 2.
- Continue this action until you get a marked change of sensation. You will not hurt yourself by repeating this action.
- If you want to, rest for maybe 10 seconds to half a minute and repeat.
- You will not harm yourself by repeating this process. Repeat until you get a result, but if you are on the spot you should get quite a quick response. But do go gently at first.
If you have access to a professional therapists they can do this:
- Bring the two ends of the muscle toward each other so that the muscle goes slack and is not stretched, for about 20 seconds. They do this to make the most of the contraction and release response which accompanies muscle movement.
- They will then gently stretch the ends of the muscle apart to move it toward its ‘normal’ resting length. Once this has occurred blood flow will be restored and the pain will stay away until the bunching and build-up of waste products occurs again.
Unfortunately you cannot do this bit for yourself as it has to be done passively because your voluntary movement will put tension back into the contracting muscle. But the pumping action will be useful and you can control that yourself.
Risks
- The main risk is overdoing it. Remember that it takes energy and oxygen to clear these blockages. I only do about 5 points to start with and see how you’re doing. I have heard of a young woman who got such relief that she urged the therapist to go on and then had a serious crash next day; so, as always, easy does it at first.
- If you go to a professional therapist you may find that getting there and back is more than the relief is worth. Be aware that they may want to give you the full hour’s treatment. Again, limit the time until you know your limits.
- And, as always, you may have to listen to some idiot therapist’s theories. There are some mighty judgmental self-righteous therapists out there. Block your ears if you hit one, and pass on the info if you find one who is useful.
Resources
This therapy is widely used by people with fibromyalgia, so there are a number of useful guides and books on the subject. These are just a few. The Arthritis Foundation may have more.
Tender point therapy is widely used in FM, but people with ME/CFS may not know about it
David Simons and Janet Travell wrote Myofascial Pain and Dysfunction: the trigger point manual in the 1950s. This was the pioneering publication on the topic and is still the classic.
Clair Davies and Amber Davies, The Trigger Point Therapy Workbook: Your self-help treatment for pain relief, (New Harbinger 2004) is clear and has good guide to locating points and self-treatment. It was written by two people who cured themselves of chronic pain (they didn’t have ME) and then trained as therapists.
Valerie DeLaune, Trigger Point Therapy for headaches and migraines: your self- help Treatment work book for pain relief, (Oakland Ca. New Harbinger 2004) has very good illustrations of common referred pain patterns relating to the head and neck.
Donna Finando: “Trigger Point Self-Care Manual”, (Rochester Vermont, Healing Arts Press, 2005). This shows various ways of reaching hard-to-reach points on your own.
Simeon Niel-Asher: “The Concise Book of Trigger Points”, (Chichester, Lotus Publishing, 2006).Very good on the location of common trigger points and their associated pain patterns.
Leon Chaitow, Modern Neuromuscular Techniques, (Churchill Livingstone, 2003 first published in 1996) is rather complex for self-help but has an excellent CD clearly demonstrating his treatments which a willing person could copy. Chaitow is the ultimate osteopath, an enthusiast for complementary therapy; he trained many therapists at Westminster University in the UK.
Leon Chaitow: Positional Release Techniques, London, Churchill Livingstone, 2007. This is another Chaitow textbook; it is not well written but develops the technique further. It has a good CD showing the use of these techniques. Other aids: Some people use a sort of stick with a knob on it (a bit like a device for throwing balls for dogs) to reach difficult sites.
Tim Parkes, Teach Us to Sit Still (Vintage 2011) may interest you. Tim is a writer who lives in Italy. He does not have ME but did have disabling internal pelvic pain. He could not sit, he could not sleep, and it was excruciating to urinate, etc. His search for an answer to this pain is told in a humane and engaging way which you may find sympathetic. The doctors offered all sorts of drastic urological surgery, which he nearly had in desperation.( I know someone who had surgery for this condition and it made it much worse, because the urinary tract itself wasn’t the problem.)
Tim Parkes has a good chapter on the ‘promiscuity’ of the internet where so many people offer promised cures, along with bogus testimonials motivated largely by having something to sell. It is best to take your cues from patient-controlled sites such as healthrising or similar.
However, while looking for an explanation he came across a book called a ‘Headache in the Pelvis’ by two Californian therapists and recognized himself (David Wise and Rodney Anderson, Popular Medicines and Health National Center for Pelvic Pain Research 2010). They suggested that the condition was caused by the development of trigger points in the muscles of the pelvic floor. The treatment they offered was trigger point therapy up the anus. Tim did not fancy flying to California to have an unorthodox ‘treatment’ applied to his bowels, but their description fitted his case and answered many questions.
So he took up meditation. He practiced the extreme form where you sit still for 10 days (how could he have stood it? Or sat it?). Anyway, by learning to really relax he did solve his physical problem, although he got a bit hooked on meditation!
The point was that the deep relaxation did help the muscles to ‘let go’ and the knots to release. So it may be that this is why things like Yoga Nedra which increase oxygen and reduce muscle tension can have such helpful benefit for ME. It is also maybe why massage and reflexology can reduce distress too, at least temporarily. The website for Health Rising (healthrising) has very useful up to date information on oxygen deficit, blood volume restriction, etc.
Myofascial Therapy
The myofascia are a film of usually whitish material that covers our organs, every muscle fiber, and each muscle. It looks like a sort of white cling film which covers kidneys or legs of lamb in the butcher shop.

In this dissection of a hand, the fascia associated with one muscle are shown in purple near the thumb
When you try to remove it it turns out to be quite tough. It is extraordinary stuff; its role is to retain the shape of our organs while allowing them to slide over each other at the same time. So it is tough, holds its shape, and is flexible–all at the same time.
The myofascia (myofacia) form a continuous sheet throughout the body, but this sheet has a characteristic pattern of ‘trains’ or lines of tension running through it. These tougher trains run up the back of the neck and over the skull and may be anchored above the eyes in the brow. You can get an idea of these trains by pulling on one corner of a jersey and seeing how the lines of tension fan out.
The reason for this is something of a mystery, but it’s possible that it is a semi-solid which can also develop lumps and knots, and maybe even crystals– especially along the trains of tension. If it gets tangled up and knotted, the myofascia can become really painful.
As with trigger points, the pain can be referred quite a distance away from the site of the tangle.
If you have been immobilized, then the myofascia may well lose their fluidity and become painful.
Therapy
Myofascial therapy is very gentle and should feel quite pleasant. It consists of a slow stretchy pull generally in the direction of the ‘train’. The warmth of the hand also helps the stretching and easing. You simply hold this pull until the material ‘gives’ slightly and straightens and stretches out. You just wait patiently for this ‘give’ to occur.
The person acting as the therapist gently ‘engages’ with the tissue, usually with the ball of the hand or the length of their arm. This should not be painful or hard; it is just a ‘holding’.
The idea is just to anchor the fascia so that your supporter or you can apply a slight slow pull against the anchor. As the tissue softens the sensation will be as if the resistance eases and you are ‘let through’. You then go on to the next bit.
It can be done in co-operation with a willing partner providing the anchor, but you may need to guide them and not let them get heavy handed.
Risks
As above. The risks seem to me to be very low, but the even the gentle pulling action will involve effort and some energy.
Therapeutic Services
The training is post-basic massage training, usually a certificate in addition to basic massage training.
Resources: Robert Schlep, Thomas Findley, Leon Chaitow et al. al. Fascia: the tensional Network of the Human Body: the science and clinical application in massage and movement therapy, is not well written but will tell you much more about the fascia.
Leon Chaitow and Sandy Fritz, A Massage Therapists Guide to understanding, locating and treating myofascial trigger points, Churchill Livingstone, 2000, is a good guide to where the tangles may be.



Dear Philida Bunkle,I am so pleased to see something written by New Zealand.
I am an ex nurse and did a dip in massage 1990s
So now I reap the consequences of having lead a busy life with the inevitable losses etc.
I use the PatientsLikeMe website And out of thousands of FM sufferers I find myself in comparrison, able to live a limited but satisfying life.
I have visited the local christchurch support group for FM but found a group of friendly elderly ladies who seemed into pills and specialists and having more worldly wealth than me! An impression only.
So I get along with swim pool,acupuncture,Helios Medical centre for supplements and minimal
meds,and some hobbies and interests.
But people do seem to recover and I am curious.Perhaps one needs lots of money to buy things or is it knowing the right people who have found recovery?for inspiration?
I have got most info from US A even if they seem to me to be drug orientated.
It seems medical care and attitudes vary enormusly from country to country,Dr.to Dr.,person to person but the internett becomes the melting pot for all facts and experiences.
Thankyou Philida for your writing and info.
Sincerely,Philippa S.
Excellent information that is clearly explained.
My understanding of how to get the blood flow through these points has definitely improved my understanding of exactly what trigger points are, how the blood flow through or blocked in them, causes the pains that I as a patient suffer.
It makes sense to anchor the fascia gently as you unblock the tender point you are manipulating. This was a new technique that your essay made me aware of.
It is understandable that anchoring ( applying tension lightly in the opposite way of the direction an area is going to be manipulated), is used in other treatments such as drawing blood, or starting an IV, and techniques that doctors learn.
It must be a physical law.
Thank you very much for writing this helpful information.
I hope you will forgive me for bringing to your attention the fact that this article did not recommend combining trigger point therapy and myofascial release, the latter considered to be a treatment in itself. According to Travell and Simons, myofascial release has limited effect in the treatment of trigger points and I believe it is a treatment which does not get to the source of the problem. Symptoms may be temporarily relieved but are usually not long lasting. Trigger points start in the muscles, spread to the fascia and then to the skin, resulting in allodynia. Getting to the source and deactivating the trigger points will result in the fascia and skin reverting to normal. I have had this experience myself. However, deactivating trigger points is not enough if all the perpetuating factors are not addressed and there is a long list of them. I also would not recommend Phillida’s mode of therapy as it is very painful and very few people would stick to it. I have used the stroking method for the last 17 years and I find it to be very effective with minimal aversion. There is a myth though that trigger point therapy will always give you instant relief and the trigger points can be released quickly and easily. OK if it is a new pain but if it is a longstanding problem, stirring up the trigger points can make it worse for a while before it gets better ( we all know the old saying). From my own experience also, the trigger points can appear asymptomatic but when you find one (and it is not nice – it is so painful it makes you jump which is why Travell and Simons called it the jump sign), working on it does not immediately illicit the referred pain pattern. This may happen up to 5 -10 minutes later ( our nerve conduction appears to be slower). I find Clair Davies book to be excellent as it gives just enough information for lay people to apply themselves to their own trigger point therapy and find a lot of success. I use a theracane and a tennis ball or lacrosse ball in a sock so you don’t lose it. Phillida mentions the work of professional therapists in stretching the trigger points out of muscles but fails to mention that the skin must be anaesthetised in order for this to be effective ( this is known as spray and stretch).
Tricia, I agree with your comments.
I have FM and myofascial syndrome as well as the above I find the microcurrent device called the Alpha-Stim helps in a gentle way of releasing trigger points.
Also using a ball and rubbing against a wall to release trigger points in the shoulders and back and lying on the floor to release Gluteus maximus. My favourite ball is a softer dog ball. posture is also essential to help stop the perpetuating factors.
The book I prefer is ‘Healing through trigger point therapy’ by Starlanyl and Sharkey. A little more detail than the others mentioned.
Hi
I’m Belgian and myofascia therapy is called just fascia therapy here. It is an ‘art’ that has to be performed by a skilled fysiotherapist. It helped me greatly and I experienced it to be much more than a mere physical therapy, it helped on an emotional and even spiritual level as well (this was also because the therapist was very, very good).
Then I took up qigong and I stopped going but I do recommend this highly.
Thanks for the book references.
Some of us with ME/CFS mainly have the neurological symptoms, such as pressure headaches, mental fog, fatigue and sometimes light sensitivity and cardiac arrhythmia. I try to exercise daily, so maybe that’s one reason I don’t have much muscle pain.
I was just reading about the symptoms of concussion and the similarities in some areas are striking. One difference is that the ME/CFS symptoms vary a lot, even in the course of a day.
Another excellent technique is instead of using a dry needle or one with a saline/ribose solution, is to inject your own platelet rich plasma directly into the trigger point. “PRP” injections as they are called puts the nutrients most needed directly into the damaged soft tissue!
Hello everyone,
I had the exceptional good fortune to be the patient of a neurologist who specialized in trigger point therapy for 12 years – Dr. Robert Gerwin. Unfortunately for his patients he retired at the end of 2013 leaving a huge gap in local medical knowledge on what remains an arcane subject. Dr. Gerwin was 75 last year so his retirement was certainly due, he did tell me that there was no other neurologist in the area practicing trigger point therapy so he was unable to make a referral.
Philida Bunkle’s article gives a short synopsis of several conditions and therapies that are otherwise very poorly understood and/or described in most of the commentary I have seen on the Internet. Trigger points, tender points, pressure point therapy, myofascial release, dry needling, injection therapy etc,etc.
I would recommend anyone interested in trigger point self therapy to get Clair Davies’ manual which is inexpensive (less < $20 from Amazon) clear and easy to follow. If possible get the first edition of Davies' book – the later editions just add extraneous information. A theracane and a small hard ball are also needed. I use a super ball as I find tennis balls too soft.
Dr. Gerwin described trigger points as adhesions in a band of muscle that would prevent that muscle from relaxing, resulting in a taught band of muscle. The trigger point can be identified as a knot or lump usually near the center of the taught muscle. Pressing on this knot is highly painful.
Trigger points can vary from painful and annoying to crippling in their effect. Anyone can get them from injuries due to sports or accidents but some of us with ME have some chronic problems. I manage most of my trigger points through self help with a theracane and a ball in a sock but for some severe ones professional intervention is required. For some reason when a needle is inserted into a trigger point it will cause the adhesion to release, which also manifests as a strong twitch in the muscle and considerable pain. The pain is short and the relief is long lasting.
Personally I have been cured from radiculitis (compressed nerve root at the spine), TMJ and a severe problem with my piriformis in one leg that was crippling, by needling, as well as several less sever problems.
After treating a trigger point it is best to apply moist heat for about 1/2 hour and follow with ice thereafter, heat to relax the muscle and ice to ameliorate inflammation. For self help this is not usually necessary.
A lot of suffering can be avoided through trigger point therapy. I recommend it highly to anyone who has chronic muscle pain. Just useful for actual trigger points though..
I hope this is useful and wish you all the best
I went to a Neurosurgeon at Northwestern Memorial Hosp. in IL about 6 yrs. ago. He had me see a physiatrist, a doctor who doe non-surgical spine and musculoskeletal care for myalgia of the neck & back & migraines. She gives me novacaine shots in those trigger point areas which help a lot. Massages were also recommended & PT. I have been using the
theracane, balls in socks & waded-up socks for years. Helps tremendously except now my hand are going (very hard to use theracane now which was my lifesaver. In the massages as with the rest you have to find the referred pain also. I was told by PT if you try to relieve the round knots or swollen glands in your necks in circular motion you bruise the tissue. They recommend long straight strokes down that will touch over the bumps so you get even tension & don’t bruise the tissue. I use the “Trigger Point Therapy Workbook” by Davies & Davies as a reference. It is a good manual for trigger points for your whole body.
It seems like we are all doing pretty much the same thing. Hopefully more relief will come along soon!
I went to Northwestern Memorial Hospital, recently. I was told to go to the pain management center. There, they work with all sorts of methods.
However, the doctor would not allow me to enter the program because I have fibro./me and I am too exhausted to exercise. He would not prescribe anything for pain because he said it would make me tired.
Well, I am already tired and in pain. I’ve been this way for 20 years. Can you tell me who was the doctor you saw or suggest another place at Northwestern Memorial? It is one of the best hospitals around.
Hi Rebecca,
I suggest try and find a doctor or therapist in your area using the Alpha-stim (microcurrent therapy). It is a very gentle way of releasing trigger points. Also if you use the ear-clips for a while you should see an improvement in sleep and therefore more energy to cope with exercise.
Or buy your own alphaStim, they are made and marketed in Texas easily applied without a therapist