
The Open Medicine Foundation released two videos of Ron Davis talking about their work over the past couple of weeks. I got a chance to talk to Davis twice since then and to flesh out a bit more what he’s doing right now.
As most people probably know, the Davis group’s working hypothesis right now is that problems with glycolysis – the process producing many of the raw materials the mitochondria use for energy – is impaired in chronic fatigue syndrome (ME/CFS). Their data is leading them to suspect an enzyme called pyruvate kinase is this issue. The Fluge/Mella group has come to a similar conclusion, but they’re more focused on a different enzyme called pyruvate dehydrogenase.
Both are coming to the conclusions in an indirect sort of way. Fluge and Mella’s amino acid metabolism results suggested problems with glycolysis were present. Davis’ experiments and metabolomics results suggest the same. Davis noted, though, that neither is directly measuring the performance of the enzymes that break down pyruvate.
Tools of the Trade
“He’s not just a one-hit wonder. He’s a frequent provider of disruptive core technologies.” George Church, Professor of Genetics, Harvard
Davis’s forte is creating new technologies. Named one of the great inventors of the century by the Atlantic, he created many of the tools that made the Human Genome Project possible. George Church, a Harvard professor, called him a “frequent provider of disruptive core technologies”.
It’s no surprise, then, that Davis has been creating new tools to help him better understand the energy depletion process he believes lies at the core of ME/CFS. Davis is guided by two ancillary goals as he does this: to make the tools as cheaply as possible to avoid the problems with funding that come with ME/CFS, and to produce “fast assays” he can use to test as many potential treatments as quickly as possible.
Indirect Measurement of ATP
Davis has produced an assay which involves bombarding cells with sodium chloride. Because too much sodium chloride is toxic to cells, they have to pump it out again. They’re easily able to do that but that process requires energy, lots of it. Davis’ working hypothesis is that cells that die when placed in sodium chloride probably die because of their inability to produce enough ATP to get rid of the salt.
Science can be messy though. The sodium chloride is triggering inflammation in the ME/CFS patients’ cells but not the healthy controls’ cells. That raises the question whether inflammation is the problem or reduced ATP production or both? It’s an unexpected twist that has to be explored. Davis noted that these kinds of twists and turns are normal in science.
Electrical Impedance
“We teach the engineers medicine and they teach us electronic circuitry. It’s a whole bunch of people learning all the time. We feel like there’s nothing we can’t do.” Ron Davis
Electrical engineers are providing the next step by measuring electrical impedance (the amount of electrical resistance) in ME/CFS patients’ cells.
This tool was produced using nano fabrication. About the size of a dime, it needs a 1/10th of a drop of blood to function. In order to account for cell movement, 2500 electrodes placed 100 nm apart measure the electrical current in the cell. How big is a nanometer? It takes an electron microscope to distinguish a nanometer and those little electrodes – you can’t see them either.
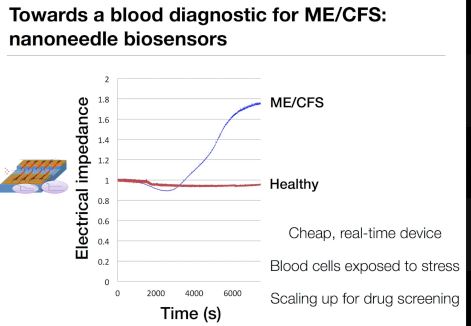
Electrical impedance rises in ME/CFS patients cells after they are stressed
These electrodes aren’t only small – they’re blazingly fast – making 200 measurements per second. By using a 3-D inkjet printer – the next step – Davis will be able to print out this tool at an amazingly cheap cost – just $.10 a sample.
Davis said electrical impedance is increased in cancerous cells and cells infected with bacteria, probably because the cells are dying. ME/CFS patients’ cells are not in such bad shape at rest, but when Davis puts them under salt stress their electrical impedance increases as well. Cells from healthy controls, on the other hand, show normal levels of electrical impedance under salt stress.
Davis’s recent finding of reduced electrical impedance levels in a chronic fatigue syndrome patient (ME/CFS) who is still working and is pretty functional suggested that he may be getting at a core part of the disease. Next Davis will look at a range of subjects including a student who had ME/CFS and is now recovered. If the cells from the recovered student – who can now run 10 miles at a time – also have increased impedance, Davis may have uncovered a hidden weakness that predisposes people to ME/CFS. He will also start doing the test in people with different kinds of fatigue including people with overtraining syndrome.
Levitating Cells To Understand ME/CFS
Davis is also using magnetism to levitate cells in glass capillary tubes. The cells float to the top or drop to the bottom depending on how dense they are.
He’s been doing this with his son Whitney’s cells for quite some time. Whitney’s cells have always proved to be quite light; they float right to the top of the tube. Davis isn’t sure why this is, but he suspects that it could be because the glucose in Whitney’s cells is getting consumed and being turned to fat – a lighter substance.
Cancer cells also display this characteristic. Again, Davis believes that as cells begin to die their density may drop.
This is another astoundingly cheap (5 cents/sample) test; the tool simply needs an IPhone to do its work. It takes about 10 to 20 minutes and could easily be done in a doctor’s office.
Finding the Culprit – the Serum Studies
“If it is in the serum, we probably can find it and that is what we’re trying to do now, which is find the component or components – most likely plural – that is causing this effect… Now this a good hypothesis, and we are now testing it.” Ron Davis
Davis can potentially get at what in ME/CFS patients’ serum is causing ME/CFS or healthy cells to be so lethargic in a couple of ways. He can add things to or filter out substances from the serum and see if the cells return to normal; i.e. have normal electrical impedance levels.
Thus far Davis have found two substances, pyruvate and ATP, which allow their cells to act normally. Unfortunately neither of these are possible candidates for treatment. In fact both could make patients ill or even kill them.

Davis’s working hypothesis is that the answer lies in the blood – and that it’s findable..
Pyruvate could be providing the energy the cell needs or it could simply be blocking whatever is blocking the pathway now. Because pyruvate is not very soluble, it would be hard to take enough do any good, and in doing so might cause other problems such as bacterial overgrowth or increased lactate production.
As Davis learns more he’ll model the effects of pyruvate on ME/CFS patients in order to learn what it might be doing. He believes, though, more effective substances will come along.
ATP plays the role of a signaling molecule outside of the cell and could make people quite sick or even kill them if they were to take it in sufficient quantities.
As Davis finds substances which increase the energy status of ME/CFS patients cells he’ll test these other substance in people with other fatiguing illnesses such as overtraining syndrome to see if they react as well.
Treatment
As noted earlier Davis’s tools are being produced in service of a goal to rapidly assess the effectiveness of scores of drugs or compounds in chronic fatigue syndrome (ME/CFS) patients cells.
His literature search has given him a set of factors that could be elevated or depressed in ME/CFS patients’ cells. Another search has given him a list of drugs that could impact those factors. Plus he has samples of virtually every FDA approved drug in existence that he can test in ME/CFS cells.
Currently he’s examining the effects of 96 drugs on the cells. He’s hobbled a bit right now in his inability to test large numbers of cells and substances at once using the instruments he’s developed. Fixing that problem is the next step.
A Strategic Approach
Davis’ strategic approach (so far as I understand it) to understanding and finding ways to impact the energy problem in ME/CFS patients’ cells has been the following:
(1) First he found a way to assess our cells ability to generate energy by putting them under salt stress (the sodium chloride test)
(2) He then created a tool or tools (electrical impedance, magnetic levitation) which he can use to measure their energy status or health (electrical impedance, magnetic floatation).
(3) With these two tools he can put cells under stress, add possible treatments to them and see if they respond.
(3) After tests suggested that something in ME/CFS patients’ blood was inhibiting their cellular energy production, Davis began filtering their blood to see if he could remove the substance. He found that he could and that a large molecule or protein was likely responsible for blocking the cells’ energy.
(4) Using what he’s learned about the energy production problems Davis began to add substances to the serum to see what would allow the ME/CFS cells to tolerate the salt stress. He’s found two substances so far. He’s also begun to test those substances in a wide variety of patients and people with other fatiguing illnesses to determine if the same issues are present in them.
(5) Davis also used the scientific literature to come up with a list of drugs that might help. He’s testing about a hundred of them in the serum now.
(6) A next step is to be able to create the ability to quickly test many numbers of cells and substances at once.
(7) Drugs or substances that pass the test will give him clues about what’s going on and will provide the foundation for further tests. A variety of problems may be found.
A Drug Target
Ultimately Davis is looking for a drug or other substance that can turn ME/CFS patients’ cells back on. (Davis is on board with Naviaux’s idea that something is keeping the cells in a hypometabolic state.)
His finding that a large molecule or protein is probably responsible, and is hopeful because that kind of molecule is a perfect target for a drug. That drug – which no one probably has ever connected with ME/CFS before – could be sitting on a drug company’s shelves, somewhere.
Davis noted that drug companies have produced thousands of compounds that never made it to market. The market may have been too small to justify the cost of expensive trials or the side effects may have been a problem or the drug just didn’t work in that patient population. A significant number of drugs have already gone through Phase I (safety testing in humans) and Phase II (efficacy and further safety testing in humans) trials.

Could a drug that could work for ME/CFS be sitting on a drug companies shelves?
AZT is a glaring example of a drug that was sidelined for years but which laboratory tests (much like Davis’) using a similar procedure suggested could be helpful for HIV-AIDS. HIV researchers put AZT in HIV-infected cells to see if the virus went away. Davis is putting compounds in cells to see if the cells act normally when put under stress. It’s the same basic procedure.
Davis suggested that an effective drug for ME/CFS might just end up being a complete surprise – a drug that no one has ever considered might work. He doesn’t, by the way, think that people with long-term cases of ME/CFS are lost. While changes in the illness may occur over time, he believes that if their systems have been reset once they can be reset again and recovery should theoretically be possible.
Davis also doesn’t believe that the protective mechanism that Naviaux (and he) believes is keeping the cell in a hypometabolic state is protective any longer; he thinks a switch got flipped on that should have gotten flipped off and never did.
In fact, if Davis and Naviaux are correct, then the right drug might not just temporarily correct ME/CFS but could solve it permanently simply by getting the body back on the right track again. In this scenario you don’t take a drug again and again and again. You take it once or enough to reset the system so that it proceeds normally.
In the recent video Davis also presented the hypothesis or possibility that trying to push through ME/CFS symptoms has kept Naviaux’s alarm system on. Davis didn’t elucidate more on this hypothesis, but you could envision a scenario where Naviaux’s danger response gets invoked as ME/CFS patients try and push through their illness. The danger response’s response, of course, is to then inhibit the energy production of the cells.
Picture this happening time and time again – each time the danger response clamping down on the cell’s energy levels more and more. Picture it happening so many times that the danger response has so inhibited energy production that a person becomes bedbound. That, at least, is my interpretation of what Davis suggested could be happening.
NIH Research Center?
Like all ME/CFS researchers, Davis needs money and he’s going to apply for an NIH funded ME/CFS research center grant. Each ME/CFS research center will get about 1.2 million dollars to play with. The university the centers are attached to will, if I got it right, also get about $800,000 a year in indirect costs. If those numbers are right (about $2 million/center) we’re looking at three NIH funded research centers coming into being over the next year.
Two hundred thousand of that $1.2 million will go to a collaborative project all the research centers will work on. Some money will get eaten up by the stiff reporting requirements.
Some will also get eaten up by the collaborative nature of the grant. The NIH wants the research centers to collaborate with outside institutions, but that’s going to come at a cost. Each research center will be responsible for the indirect costs (@40%) it has to pay to the university the researcher it’s collaborating with is associated with. (If an outside researcher is paid $300,000 for a project, the University will get an additional $120,000 or something like that. That money will get paid out of the $1 million dollar grant for the Research Center.
With that we’re down to $850,000 or something like that a year that each research center will have to use on its own projects.
Davis’ grant application will contain a long list of researchers he will be collaborating/consulting with. (Indirect costs do not need to be paid to consultants/volunteers). It’s a pretty heady mix of collaborators/consultants. (notice Davis’s propensity below to attract researchers who have their own labs.)
If the grant is awarded purely on the strength of the team each researcher can enroll, Davis may very well come out on top. He’s drawing from Stanford, University of Utah, Harvard and other universities. He’ll get his patients from Dr. Montoya, Dr. Bateman and Dr. Levine.
Stanford
- Mike Snyder, PhD, Chair of Genetics Dept, head of the Snyder Genetics Lab at Stanford, Director – Stanford Center for Genomics and Personalized Medicine
- Craig Heller PhD, Biology Prof, co-director of the Stanford Down Syndrome Research Center and director of the Craig Heller Lab
- Mark Davis, PhD, Chair of Immunology Dept, head of the Mark M Davis Lab at Stanford
- Catherine Blish, PhD, Asst Prof, Immunology, NK cell expert and head of The Blish Lab at Stanford
- Laurel Crosby, PhD, Research Assoc, Stanford
- Raeka Aiyar, PhD, Molecular Biologist and Communications Director, Stanford Genome Technology Center
- Jennifer Frankovich, PhD, PANS Program Director, Stanford Children’s Hospital
- Rahim Esfandyarpour, PhD, Research Engineer, Stanford
- Fereshteh Jahaniani, PhD, Geneticist, Research Associate, Stanford
- Peidong Shen, PhD, Chemist, Research Associate, Stanford
- Jose Montoya, MD – Director of Stanford Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Initiative
Utah
- Baldomero Olivera, PhD, Director of Olivera Lab at University of Utah
- Mario Capecchi, PhD, Molecular Geneticist, Director of Capecchi Lab at U Utah, 2007 Nobel Laureate
- Alan Light (PhD) and Kathleen Light, (PhD), U Utah
- Lucinda Bateman, MD – Bateman Horne Center – Salt Lake City, Utah
- Suzanne Vernon, PhD – Bateman Horne Center – former Research Director of CAA, CDC ME/CFS researcher
Harvard
- Wenzhong Xiao, PhD, Physical Chemist and Bioinformatisist, Director, Inflammation & Metabolism Computational Center, Harvard professor
- Ron Tompkins – Professor of Surgery, Harvard
Others
- Curt Scharfe, PhD, Geneticist, mitochondrial expert, professor at Yale
- Robert Phair, PhD, Biochemist, retired from Professorship at Johns Hopkins, now CEO of Integrative Bioinformatics
- Mohsen Gorgani, PhD, Biochemist, retired
- Susan Levine, MD – New York
It’s a lot of people – easily enough people for a $5 million a year grant – which is exactly what Davis hopes to see over time. Davis hopes that the level of the funding award increases soon. He pointed to the fact that Vickie Whittemore (whom he and others praised) said one of the difficulties raising money was that by the time the effort got started the NIH Institutes had allocated their funding for the next three years. That meant the Institutes had to raid other diseases to get their funds.
That suggested that by the time the Trans NIH Working Group got its program together and jumped through a few hoops, the $2 billion dollar increase the NIH got had already been allocated.
Thinking Outside of the Box
“I wanted the most out of the box thinkers I’ve ever met. I made a list, called them and they all said yes.” Ron Davis on the OMF’s Scientific Advisory Board
 Davis is a fan of thinking outside the box. Our thinking is often limited, whether we know it or not, to certain options and possibilities. Because thirty years hasn’t gotten us to where we want to be in ME/CFS, Davis suggests it’s probably time to think differently – to have the courage really – to look outside of the box and entertain new possibilities.
Davis is a fan of thinking outside the box. Our thinking is often limited, whether we know it or not, to certain options and possibilities. Because thirty years hasn’t gotten us to where we want to be in ME/CFS, Davis suggests it’s probably time to think differently – to have the courage really – to look outside of the box and entertain new possibilities.
That brought to mind the parable of the man searching for his keys.
A police officer sees a drunken man intently searching the ground near a lamppost and asks him the goal of his quest. The inebriate replies that he is looking for his car keys, and the officer helps for a few minutes without success. Then he asks whether the man is certain that he dropped the keys near the lamppost.
“No,” is the reply, “I lost the keys somewhere across the street.” “Why look here?” asks the surprised and irritated officer. “The light is much better here,” the intoxicated man responds with aplomb.
One example of thinking outside of the box is to think of fatigue differently. Fatigue has understandably come to be something of a bad term in the ME/CFS community, but fatigue is a very common outcome of chronic diseases. Plus, because fatigue is potentially able to affect every cell and organ in the body, it’s possible that in some ways it could underlie many diseases. Davis asked Francis Collins, the director of the NIH, how he would feel if ME/CFS turned out to be the answer to many diseases and Collins missed the opportunity to study it.
Davis wonders if the fatigue in chronic fatigue syndrome (ME/CFS) could be of a special kind. In other diseases, patients may have a type of fatigue that doesn’t allow them to exert themselves – hence they have limited post exertional malaise. ME/CFS patients, on the other hand, may have a type of fatigue which allows them to over exert themselves – hence the extreme problems with PEM. (So far as I can tell the term PEM didn’t exist before ME/CFS came on the scene).
Davis isn’t saying that this is true – it’s just an idea. It’s a way of thinking outside of the box. Another example of this concerns the Institute at the NIH ME/CFS belongs in. We’ve long thought that ME/CFS should belong in either the immune (NIAID) or nervous system (NINDS) Institutes, but if the metabolic abnormalities hold up it’s possible ME/CFS might fit better in the (NIDDK) National Institute of Diabetes, Digestive and Kidney Diseases.
A New Field Emerges? The “Haplogenetic” Study
Another example of thinking outside the box is the Open Medicine Foundation’s (OMF) genetics/metabolomics study that’s being done in collaboration with Dr. Naviaux. The study will explore a novel hypothesis Davis has come up with that Davis’ partner, Janet Dafoe, has termed “haplogenetics”. It involves a situation called heterozygosity which occurs when one copy of a gene (we all carry two copies) doesn’t work resulting in that gene producing only 1/2 the normal amount of protein that it usually does.
Ordinarily that’s enough, but Davis wonders if increased levels of heterozygosity could result in a hypometabolic disease like ME/CFS. If, for instance, NAD, a coenzyme vital to the energy production process, is low across the board, it would affect many metabolic pathways. Other heterozygous genes could help explain the heterogeneity present in the disease.
Researchers Ready to Engage – If the Funding is There
From day one,of course, Davis has been working on getting outside researchers involved. When I asked him what the reception has been like, he said that everyone he’s asked has been interested; there’s something to exploring the unknown that’s tremendously exciting to good researchers. Throw in the possibility that they may be uncovering basic biochemical pathways in the body and you have some real interest.
Plus Davis has done this before with the Human Genome Project and the sepsis project. He’s good at tackling big questions and creating collaborative environments that give creative minds the room the grow.
The OMF’s Severe ME/CFS project is funded, but Davis’ possibly most exciting work is still being done on a wing and a prayer. He’s jury-rigged a project that is almost entirely dependent on volunteers. He’s got some great volunteers – electrical engineers, geneticists, immunologists, etc. – but you can only do so much volunteering your time.
His program, like others, is crying out for dedicated funding. In the Q&A video Davis said that in order to do what he did with the Human Genome Project, to really attack the problem with skilled researchers he needs $5 million/year for multiple years.
It’s not a lot of money. Surely people exist in Silicon Valley or elsewhere with relatives or sons or daughters with ME/CFS who could contribute $1,000,000 a year for five years or ten who could contribute $500,000 a year.
When I look at what Davis is doing with his limited funds, I wonder what more he could be doing with a dedicated team devoted 24/7 to figuring out what the heck is going on. I wonder what we are missing by not giving those fertile minds the opportunity to do that. That’s a question every potential donor with deep pockets might think about.
I propose that one person step forward and state that they will commit to providing Davis a million a year for five years. Then perhaps four more people will step forward and do the same – and we will see what happens. At $5 million a year you’re not working around the edges anymore, you’re not cutting corners – you now really have a chance to make a difference. That’s exciting stuff.



Hello my name is Leon Pogorelis i live in Hallandale beach FL after your last video DR Davis were saying that he needs more blood samples from CFS patients DR Klimas has my blood work that was taken in VA Miami if that will help in anyway. thank you i was in DR Klimas study
How does this compare with what the Aussie team just announced in their research last week regarding calcium channels?
They seem very different. I do remember, though, that intracellular calcium levels can affect mitochondrial enzymes – so possibly there could be a connection.
I remember looking into those the business of energy generation of ION channels a few years ago. I am type I diabetic as well as having ME/CFS. There various ION channels (Potassium-Sodium, Calcium etc) each required a different threshold of energy within the cells before they begin to work.
You would therefore expect that as the energy production worsens the ION channle begin to fail in an expected sequence.
“The sodium chloride is triggering inflammation in the ME/CFS patients’ cells but not the healthy controls’ cells.”
Would this make high salt diets a problem?
I don’t know… My guess is that Davis is really hitting the cells hard with sodium – probably much harder than we do with our sodium intake. Sodium only seems to help me…
My ME doctor here in Australia has long observed that ME patients tend to retain too much sodium. My initial sodium retention test bore this out, as did my ‘puffy’ wrist and arm. A subsequent test during treatment with a drug that reduces sodium retention shows that the drug is working. That said, my wrist/arm swell more noticeably when I go into PEM; presumably indicating that the cells are ‘stressed’ (as Ron Davis puts it) by excess salt. Can’t wait to see what he comes up with next ?
What Ron is talking about is not Sodium in serum (what your doctor measures) but Sodium inside the cell and unable to get out. One should have more Potassium inside the cells and more Sodium outside cells. The cell has a special electrically powered channel to exchange Sodium that is in the cells, with Potassium that’s in serum in order to acheive this. Ron disusses this issue in he video along with its energy demands.
Sodium strongly dehydrates; my condition goes quite a lot worse when I am dehydrated; I read others experienced similar worsening with dehydration; a few ME symptoms (strong bouncing headache, confusion…) do even resemble those of severe dehydration.
Among many other options, dehydration could increase both solid and liquid non-aquas components concentrations that drive inflammation?
Another angle could be that minerals relative concentrations toward each other are often as important as how much of them you have. For example: too much sodium acts different with increased potassium compared to normal potassium levels. Maybe it further disturbs the sodium-calcium balance to link it to the Australian research? Thousands of options unfortunately…
Great article, Cort!
I hope a few millionaires do rock up but in the meantime I’d urge everyone who can to donate, donate, donate, and to ask their friends and family to do the same.
I’ve donated and know lots of other PWME who are doing the same.
Cort, can’t thank you enough for taking the time to write such long and detailed articles in a lingo that we can all understand. It all sounds so promising and gives us hope for a future. Thanks again for all your hard work! Much appreciated!!!
Thanks Nat! I use these article to learn about this stuff myself 🙂
This is pure BS. Your site is getting further and further away from the cure. You take any good idea that comes along — or wants funding — and you give it credence. CFS is viral driven and hiding in the gut.
Do you have a solution for M.E.? If so, please share this. In the meantime, hope we can keep open minds since some believe in mold, others viral or even bacterials, others autoimmume, or dysregulation, and biome is one key variable that needs more investigation. But until we see convergence, I am with Cort, Ron Davis who think we need to think outside the box and look broadly. If viral and in the gut, many viruses not treatable, so what are the options if gut viral issue? What treatments? I agree we need more B.S., = Basic Science.
Very clever Mark 🙂 🙂
Agree with Mark! Well said
For my wife and myself; We would say Ron is absolutely right. If it wasn’t for the antiretroviral isentress, we would probably be dead by now.
Ron,
I’m very sorry for whatever emotions (fear, frustration…) are driving your criticism of Dr. Davis, but we MUST be careful not to misdirect our anger at the good guys — we can’t afford to lose them. I think we can all agree that Dr. Davis has the most skin in the game here, so let’s show him the gratitude he deserves… please.
Honestly Ron, if someone with Ron Davis’s reputation comes along and suggests something I’m probably going to give it credence…I certainly grant, though, that the idea that ME/CFS is viral driven and hiding in the gut is a valid one as well.
I honestly have no idea how this is going to all turn out. Until we do know I think its best to keep an open mind. I think Ron would be the first to agree…
Hopefully we will learn much more over the next year. It would be nice to have some clarity.
For my wife and myself; We would say you’re absolutely right. If it wasn’t for the antiretroviral isentress, we would probably be dead by now.
Sorry for whatever you’ve experienced that makes you feel the need to lash out and bring others affected by this illness down. In this case Cort, with his site, and Dr Davis.
If you know the cure – you must think you do, from what you’ve posted – please set up a site or platform for expanding on this, ideally without attacking others.
When ME/CFS was first diagnosed, it happened at Lake Tahoe – you all know the story. Viruses are at the core of the issue. I’m not trying to dismiss anything Dr Davis is stating because the low energy and fatigue are at the center of mitochondria disfunction. However, one of the things I was required to do besides initiating treatment with antivirals is to increase my salt intake and lower/eliminate sugars from my diet.
I think the role of viruses in the mitochondria disfunction needs to be kept at the center/forefront of the investigation. Are we asuming that at this point of the research discussion all viruses have been eliminated? I don’t see an specialist in infectious diseases in the research team though. Am I thinking way outside the box?
Thank you for the article and summary of Dr Davis research. Very informative.
Viruses are a big part of M.E. Not necessarily in the gut though. You can fix your gut health completely and still have systemic infection of viruses and other pathogens in the body. Infection in the brain is the worst of it.
Damage can be done to mitochondria from pharmaceuticals and other toxins. Valproate made me too fatigued and too sore to work. It damages mitochondria in people with low glutathione (mine was very low).
Why isn’t there thorough testing done on cadavers of people who had M.E? It is the only way to reliably find the infections involved.
Then you need to do some research on mitochondrial damage….many people are diagnosed with fibromyalgia, Parkinson’s, CFP, MS…and what has happened to many, is that they are suffering from fluoroquinolone toxicity, which damaged the Mitochondria.
BRAVO, Cort!!!!!
Thanks
Great article. Thanks so much Cort, for all you do!
Thank you, Cort, for making the indecipherable a bit easier to decipher. Non-scientific brains appreciate the translation!
I’m sure you all have discussed this elsewhere, but given the number of Ehlers-Danlos Syndrome sufferers with worsening ME/CFS symptoms, esp among females and by menopause, who fit the profile of “overexertion”/PEM, what is the role of connective tissue in all of this? Could someone point me to any work this collaborative group is doing with EDNF? They’re coming out with an new “nosology” on March 15. It’ll be interesting to see if EDNF researchers are headed in any of the same directions.
I am also an EDS/fatigue/fibromyalgia/psoriasis/hypothyroid pt. Worst symptom is fatigue.
Thank you Cort for this excellent write-up on the video talk. Dr. Davis mentioned the use of mTOR Inhibitors in this latest video. I listened a few times to this section but could not discern if he was cautioning against the use of mTOR Inhibitors for ALL ME/CFS patients or just a subset that may have mTOR gene mutations. He said – “You don’t want to take something that inhibits mTOR…” I am surprised and dismayed about this statement and really would like additional clarification…because I just started taking Rapamune (Sirolimus) which is an mTOR inhibitor, about a month ago and have experienced SIGNIFICANT improvement in both physical and cognitive functionality. Nothing else changed in my regimen during this time. The oncologist/hematologist who prescribed this drug has 4 other patients that are taking Rapamune and all have experienced the same improvement that I have. I don’t know if it will last but besides LDN, it is the only thing that has moved the needle for me. Anti-virals did nothing for me. I posted about about Rapamune in another thread (the guy with the Castleman’s disease) but want to keep with this thread because of Dr. Davis mention. Anything you or others can add would be appreciated. Or is there an email I can contact Ron or Linda Tannenbaum directly for clarification? Thanks.
I actually had something about the mTOR subset in the original blog but took it out. As I remember Davis has found two patients with mutations in the mTOR gene involved in energy production, cellular stress and other factors. The reason I didn’t put in is that my assumption is that that mutation is quite rare in ME/CFS patients. I remember Ron saying that he had found mutations in a couple of patients in the severely ill study. While those mutations might very well be causing those patients problems they had no impact on the other patients.
So I think he’s referring to a very small subset and would probably be really interested in yours and other experiences. Davis’s serum findings suggest that a protein such as an autoantibody may be whacking the energy production system in ME/CFS. If it is an autoantibody then an immunosuppressive agent could be very helpful
I remember your comment on Rapamune in the Castleman post but I can’t remember how it came to be that you are taking that drug. (???) It’s fascinating to me that you are experiencing given Fluge and Mella’s experiences with two other immunosuppressive drugs – Rituximab and Cyclophosphamide. I don’t have a clue what these three drugs have in common but in general it’s very interesting….
Thank you Cort. Your assessment was my takeaway also but wanted to check your thoughts. The doctor who prescribed Rapamune is my husband’s hematologist. I was too ill to accompany him on his visits so we used FaceTime so I could listen and ask questions about his condition. One day hubbie explained why I was unable to be there and Dr said I should come see him and mentioned treating others with my symptoms with Rapamune with success.
I knew this relapse was different from others and that for 2 years my immune system was way out of whack and inflammation as result made sense to me given Fluge and Mella research as well as Jarred Younger hypotheses and other researchers writings. Apparently one of this Dr patients came to him with a stack of research asking if willing to work with her with immune suppressant.
The others he was seeing for other medical challenges but who also had me/cfs. All are improved. This is a very highly respected oncologist in the Dallas area and apparently an outside the box thinker. I will keep you posted on progress which I pray continues! i would love to hear of any others on immunosuppressants.
Really interesting. I’m going to email you.
Marcia, you can use this email to put questions to Ron Davis:
MECFSResearchQuestions@gmail.com
I too am very curious, would love to here more, and Cort thanks once again!
Thank you Sasha!
Sasha, thank you so much for the Ron Davis contact information!
Hey Marcia,
Can you give an update of your Rapamune story? Did if continue to work, did you stop using it?
Idk if you will ever read this since it‘s kinda old now 🙂
One more question which came to my mind is the dosage your doctor recommended? Like Jeremy once weekly something like 6mg or did you use it daily taking 2mg?
All the best and Kind regards
Samuel
“Davis is a fan of thinking outside the box. Our thinking is often limited, whether we know it or not, to certain options and possibilities. Because thirty years hasn’t gotten us to where we want to be in ME/CFS, Davis suggests it’s probably time to think differently – to have the courage really – to look outside of the box and entertain new possibilities.”
Honestly I don’t see this as the problem at all. If anything, the recent research has validated the thinking of beyond the past 30 years back well into the ME days. The main problem is and always has been lack of funding for large scale research to test out the well thought out hypotheses that came from direct observation of the disease.
First of all-thank you for all the information you provide to us about the research that is going on. It really helps to understand our illness, and give hope!
After I read about the low energimetabolism in the brain cells, and the high lactate levels that have been measured, I started to take half a spoon of NaHCo3 powder in a glass of water morgen and eve. My main symptoms has been low mental energy and cognitive problems. I have experienced an improvement in mental functioning that has made my daily life much easier. Any comment?
Thanks, Cort for this clear explanation of Ron Davis’ work. I’ve been watching his videos but haven’t known enough about the background to his work to really understand it. I do now, I think.
It’s said that we are all exposed to lots of bacteria and viruses but the reason we don’t succumb to all of them is due to the state of our own health at the time. I’m wondering if ME/CFS can be triggered by different events – viruses, bacteria etc. all of which can cause the flicking of the same switch, in people who have particular physical characteristics. What do you think?
I think most researchers probably think something like that is going on: some stressor triggers a similar kind of reset in everyone no matter whether what the stressor is…Different stressors – same general pathways. I don’t know what’s going on in the non-trigger crowd such as myself – there was no visible trigger or infection or stressful event for me.
Maybe you didn’t see it but it was there 🙂
Thank you for your great effort bringing us the latest and complex Ron’s reseach.
I can’t understand the people who think that Ron Davis is clueless.
This is not an ideologic competition, we all are in the same boat and as Cort said, it probably is the same mechanism with different triggers.
So let’s these brilliant researchers at Stanford do their job!
DOES anyone know if it would it be safe to take ATP TABS? EG:
https://www.amazon.com/Douglas-Labs-ATP-20-60-Tablets/dp/B000SVIO4A
thanks not sure if it’d be apt
I don’t know, except that I take d-ribose for extra ATP and do really well on it. Argh, confusing!
A useful blog, thanks, Cort.
“Davis said electrical impedance is increased in cancerous cells and cells infected with bacteria, probably because the cells are dying.”
I didn’t see that in the videos (I’ve only read the transcripts) – only a reference to bacteria showing increased impedance after treating with antibiotics, no mention of cancer cells). Did he say that somewhere else? I know he’s talked about this technology before.
Thanks
It wasn’t explained very well. When an anti cancer drug is added to a cancer cell the impedance goes up. They can test for effective cancer drugs this way. If the drug isn’t effective the impedance stays the same. Also for bacteria. If they add an antibiotic to a bacteria the impedance goes up, unless the bacteria is resistant to the antibiotic. You can see how amazingly useful this assay is!
Thanks for the clarification, Janet.
I am so desperate and ill that I would like to give him a real chanse. But how are we going to get the money that he really needs? 5 millions for 5 years? I can donate, we all can donate but 5 millions? I am hopeless… untill we find the money.
The money is out there. We just need to find it. There’s LOTS of money out there.
yes, but how? there are rich people on this planet but I do not know one off them…
cort, we need a plan to get the 5 millions to ron davis. 5 million, each year for five years. Otherwise he wil never get the money.
I am so ill and my had is so bad that I almost donated to the open medicine foundation because I thought he workerd there with them. My brain is so bad, can you explane me please what the diference is between the OMF and what ron davis does?
Hi Konjin
Ron is the Director of the Open Medicine Foundation Scientific Advisory Board. They are funding his work and Dr. Naviaux’s. http://www.openmedicinefoundation.org/scientific-advisory-board/
Ron does have his own foundation but I’m sure most of his money comes from the OMF.
This is from the OMF’s FAQ page:
“Thank you for wanting to support the End ME/CFS Project. Our ME/CFS Scientific Advisory Board director, Ronald W. Davis, PhD, would prefer you to donate to the End ME/CFS Project here, because the project is managed through our foundation. He says: “We need more people doing research in this area. I don’t want all this money just to fund my own lab. I want to recruit other people in other labs that are specialists in things that need to be looked at.” Donating to our End ME/CFS Project directly allows us to pay these specialist labs as needed to get more done more quickly.”
Hi Cort, All of this fits the RCCX hypothesis (www.rccxandillness.com) more and more. I have stopped reaching out about it because the idea of an exaggerated stress response seems to be unpopular, esp from a psychiatrist. That said, maybe people will be more open now.
I think there are several paths to get to this cell danger response switch and one is hetero or homozygosity for co-inherited RCCX mutations (hypermobility: TNXB, acute stress response/sex hormone issues: CYP21A2 and autoimmune diseases:C4.) We know carriers for CYP21A2 mutations have an exaggerated stress response, low baseline cortisol and possibly a stress vulnerability in the form of a switch triggered by prolonged stress which shuts off ability to make cortisol, causes salt wasting, causes 17OHprogesterone build up (with sleepiness and orthostasis) and could turn on inflammatory cascades, starting with MCAS via CRH. Under conditions of prolonged stress, those with CYP21A2 mutations (homo for those not currently able to be identified or hetero for any) which produce defective 21 hydroxylase, rather than too little, must make more than double the amount of 21 hydroxylase of a normal person. In those people, copper can get depleted (because heme containing enzymes need copper to be produced and this stress response is in a positive feedback loop, i.e. the sicker we get the more need there is for this enzyme, the more CRH is produced, the more MCAS, the sicker we get, etc), the heme enzymes unravel in the presence of low copper, including 21 hydroxylase wheihc now really drops our ability to respond appropriately to stress.
Hetero mutations in the B methylating pathways now express because those heme-containing enzymes are unraveled, too. Severe fatigue, inability to methylate B’s, low neurotransmitters starts happening, abnormal heme in urine (pyroluria), abnormal heme in brain (MS). The Naviaux/Davis cell danger response gets initiated because the body is very stressed (with or without the copper depletion and this happens in others-nonRCCX- as well). Then you take bioactive copper (which is helping many with this profile) and the enzymes work, the cortisol shoots up way above normal and in some people, this causes the 21 hydroxylase switch to trip again and 17OHprogesterone builds up again.
This is what happened to me-I am sure of it. I use berberine to lower this 17 hydroxyprogesterone. As a psychiatrist and a patient, I noticed a psych profile and exaggerated stress response in people who later develop chronic illness which I call CAPS (CYP21A2 mutation associated neuropsychiatric spectrum), a brain wired for danger, I believe due to the presence of the hormone milieu created by CYP21A2 mutations in utero and in infancy. It is also associated with sex hormone abnormalities, high adrenaline, often perfectionism, special abilities and sensory sensitivity, etc.
Many overlapping features with Highly Sensitive Person described by Elaine Aron. We are sensitive to our environment, intially over react to stress (can be very adaptive if not too much, in terms of hyperachievement) but then push through what we should not because of the high adrenaline, perfectionistic tendencies and special abilities. Right now, we can only identify about half of the CYP21A2 mutations, even with WES (can have up to a million base pair insertions and pseudogenes) and less of the TNXB mutations which I believe cause a wide range of connective tissue expression (from stiff to hypermobile). Please contact me if you have any interest in talking about this hypothesis. Sharon Meglathery MD
Thanks Sharon…I’m glad that you got in contact. I’ve been trying to find your hypothesis again 🙂
Thank you, Cort! I know how busy you are as I read your blogs. I forgot to mention that we KNOW 10% of the population are carriers for CYP21A2 and those are the known mutations. I think only about half ar known from what I can tell.
Hi Sharon.
Very interesting.
So you need to take chelated copper now regularly.
Sharon, Thank you for this. The “exaggerated stress response” caught my eye. I wonder how many of us with CFS/ME qualify as 1) Highly Sensitive Persons, and 2) have some form of PTSD.
I think that theory makes a lot of sense!
And one may not even need a mutation in those genes if they have epigenetic modifications that significantly decrease the transcription of the enzymes & increase cytokine transcription in response to stressors.
Children of mothers who were stressed significantly during pregnancy as well as kids who were abused growing up have different HPA axis responses & higher cytokine release with stress via epigenetic mechanisms.
CFS also clusters in families with autoimmune diseases, and autoimmunity can cause stress during pregnancy in the form of inflammation.
I’m curious about HDAC inhibitors — to see if changing one’s epigenetic landscape could fix one’s succeptibility to CFS & stress for good.
I am this patient. After yet another health problem and another in the past few months, I came upon Sharon’s work last week. I knew that was me immediately. I came upon the phoenix rising website and Davis’s work today searching for more helpful information. I finally came upon ME as an explanation for my newest issues, in addition to confirmed POTS, and in the midst of a workup for MCAS and hEDS. I am currently on medical leave. I am(was?) working in medical research. This has spoken to me, and I will take up the cause in my patient population, but I want to thank all of you so much for what you have done. I feel like there may be an answer and a possibility of recovery for people like me. I can’t thank you enough. If I do recover enough, you may also help me in continuing my research. I just wanted to remind you all that what you do not only helps us, but reaches the people we touch as well.
That’s great to hear Amanda 🙂 I will have an interview with Sharon coming up shortly – at least I hope it will be shortly (lol) – but it is coming.
Dr. Meglathery, I read your hypothesis. I agree with you. My mother had a very reactive, undiagnosed personality disorder. We were catholic and southern, so there was no psych performed. She was extremely high strung with evidence of mitochondrial illnesses throughout her life. At 2 yrs of age, she got the measles and responded with hypercoagulability which caused kidney failure and spent a year in the hospital. She was the type of human that considered to overreact to everything and in turn had very little support and friendships. Living with her was extremely stressful. She later developed diabetes without looking like the typical patient who is usually significantly overweight; then stroke; then kidney failure. Very stressed, reactive, and sick for her entire life. So is my brother and his child. I have been able to “hide” my anxiety taking that negative energy and put it into obsessing about school and work. I pushed forward and excelled in school, work, etc, until month’s of stressful events and a flu-like illness started by MECFS symptoms at 35 years old. Looking back, it is likely I may be an undiagnosed Aspergers. I married someone who has Aspergers and wouldn’t you know it, he began to develop dysautonomia symptoms after a Covid infection. How does one chase this theory? Is there a way to be tested for these genes? Are there medications or supplements besides the berberine and Chelated Cu supplements that are helpful?
Hi Emily, my email is info@rccxandillness.com And I run a Facebook group, called RCCX and chronic illness discussion. Feel free to reach out or join. Sharon Meglathery MD
Something that needs to be figured into the CFS equation is that women are 4 times more likely to have CFS than men – CDC info. Both men and women get their mitochondria from their mothers. So, I would think that basic metabolic/ mitochondrial flaws may result in a more even sex distribution of CFS? Despite the news from Australia and Stanford , I am still in the “structure and function” camp. Specifically, women have wider, inherently more unstable pelvises. Changes in the mechanics of the sacrum and pelvis influence the craniocervical junction, tension on the dura-meningeal system( and blood-brain barrier permeability), with the potential to create the immune, hormonal, circadian, dysautonomia that plague our lives. This happened to me. Also, this theory may explain why EDS/hypermobile people are so susceptible.
Hi Merida
Interesting ideas I think but how do you know that is what happened to you? Did you get some recovery by working on those issues in a “structure and function” manner?
I feel like this answer is easy. Women have periods and pregnancy. These are extra stresses that men don’t have. Adding the changes in women with excess androgen exposure in the brain discussed on her website accounts for the rest. The explains the penetrance is likely a matter of epigenetics.
Cort, thank you so much! I spend a lot of time attempting to keep up with and decipher the research being done – by Ron Davis, Naviaux, also in Norway, Aust etc – and it gets overwhelming. Your articles are so informative and understandable, very helpful. And Ron Davis is, I think, a hero! Thank goodness for him and his work.
Also very interested in some of the comments – especially from Sharon Meglathery and the info on Rapamune from Marcia Adelman. Would love to see some follow up on these areas.
Thanks Lauren…I’m really interested in both Sharon’s hypothesis and Marcia’s experience. Trying to get an interview with the doctor. 🙂
Hi Cort (and Sharon),
Thank you as always, Cort, for your fine work.
Per Sharon’s comments, one person asked above about taking chelated copper. I’m also wondering about the berberine she mentioned. Is that something we should be considering trying? Any thoughts re experiences with either? Are there any recommended dosages?
Again, many thanks.
Cort – I am continuing to improve significantly on the Rapamune. Last 2 days have been best so far in over 2 years. Not only out of bed ALL day but out of the house to hair salon and mini shopping. Growing in stamina too. Honestly I am shocked and waiting for the other shoe to drop, it is that remarkable. I did not expect such improvement so quickly. I hope you are able to speak wit/h Dr. Davis and clarify the mTOR inhibitor cautionary comment. I know we are a heterogeneous group with different triggers and symptoms so mTOR inhibitor may not be for everyone and could depend on length of illness, onset type, inflammation levels, immune dysregulation, co-morbid conditions etc. … but it is working for me now and I hope it might help others with similar symptoms and etiology. BTW follow up basic blood work is good so no problems yet with the Rapamune affecting liver/kidney function. And I am further encouraged as I have read Klimas and others state they expect the helpful drugs to come out of the cancer treatment community! Thank you again for reaching out with questions.
Thank you! It is so exciting to see this critical work gaining some momentum. Your article does a great job explaining. For all of us chronic illness patients who have been told for so long that we are making up our symptoms, this is an incredible breath of fresh air.
I’ve had cfs for close to 20 years. I’ve battled a number of autoimmune issues sinch early childhood. Recently, I was diagnosed with IGG deficiency and just begun in home therapy. My question is, do you see a link of CFS with these medical issues, and if so, by replacing the immune deficiency play a part in recovery from CFS?
Thank you for filling us in on some detail with Dr. Davis’s exciting work.
Just a thought – the Bill and Melinda Gates Foundation is interested in helping with neglected diseases.
Could they be a potential funder for the OMF research?
I’m slow to comment on this, but I’ll put in my 2 cents worth. I’m an almost Ph.D. (derailed by ME/CFS) biomedical researcher who has had ME/CFS for 23 years. And in my opinion, this is astonishingly good stuff which should absolutely be on this site. (And no one should be going after invaluable, hard working Cort about pretty much anything!).
Hi! At first video DR Ron Davis said starting from 12 min that
serum from healthy people made CFS patient cell to work normally. And vice versa serum from CFS patient made healthy person’s cell work like CFS ill person’s cell ?
If so, does this mean that if CFS patient donate one’s blood to blood bank then someone healthy person can come sick for CFS if this blood is transfered to him/her for example at surgery ?
Great work.. … we should contact Mark Zuckerberg who tries to invent new devices for the health system.
He has the money for more innovation and davis a good idea.
Has Ron Davis mentioned thiolate? or thiols re aa’s?