


Thanks to Amber for her striking blog proposing ways to support the very severely ill when they are at their most vulnerable state. (Images added by Cort)
This is the 2nd in a series of blogs published on HR that is focusing on the very severely ill.
- What is Whitney Dafoe’s Extremely Severe ME/CFS Story Telling Us? – Health Rising
- We are Failing People with Very Severe ME/CFS
The point of no return

The goal: preventing the very severely ill from slipping through the cracks and reaching a point of no return.
I have advocated for three people with very severe myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) in the past few years. Each time I experience the same sense of frustration, dread, and panic over my inability to connect the dots required to pull someone back from the brink. In this piece, I highlight some of the common shortcomings I have experienced in my advocacy efforts and offer ideas on how we can better support people with very severe ME/CFS.
The primary goal is to prevent patients with severe illness from slipping through the cracks and passing the point of no return. Sadly, this seems to be the trajectory for many people with very severe ME/CFS.

A harrowing experience
On January 22nd, 2021, I woke to a desperate message from a dear friend with very severe ME/CFS, who I will call Theo, informing me that he was in a 72-hour psych hold. His family had taken him to the hospital for ongoing rapid weight loss and malnourishment, likely from unmanaged mast cell disease, a common co-morbidity in ME/CFS. Rather than getting the care he needed, the hospital threatened him with involuntary commitment.
The hospital did some routine blood work, endoscopy, and colonoscopy, all of which came back primarily negative, though there were signs of slow motility in the small intestine. Rather than digging deeper, the hospital doctors concluded Theo was suffering from mental illness and submitted a petition for civil commitment (called sectioning in the UK). The hospital fought back against the recommendation of the pre-petition screener, who advocated for my friend to be released. They reasoned that Theo was a suicide risk, even though he sought medical care for his rapidly declining health, hardly the behavior of someone wishing to end their life.
This case captured the attention of several high-profile ME/CFS clinicians, researchers, and advocacy organizations from the United States and the United Kingdom. Friends rallied to raise funds and offer advocacy support. A team of us worked tirelessly on the legal and medical aspects of his case. We encountered many unnecessary roadblocks, costing us valuable time.
After three weeks in the hospital, my friend prevailed and returned home but arrived in a much more precarious state. He is now fighting for his life.
Common themes facing people with very severe ME/CFS
People with very severe ME/CFS can become isolated. As families, friends, and doctors slip away due to indifference, doubt, and overwhelm, patients have to manage their care precisely when they need help the most. In the absence of assistance, very severely ill people continue to decline until they reach a state of medical crisis and land in the ER. Instead of getting appropriate care, these frail patients often are threatened with involuntary commitment.
Any meaningful advocacy on this topic will require the input of many people, including patients, physicians, family members, caregivers, and advocates. This document represents my perspective and is based on my experiences alone.
-
Gaps in existing resources on ME/CFS
The first roadblock Theo and I faced was the absence of concise statements from authoritative sources that address the very severe end of the disease spectrum. There are many informal sources on ME/CFS, but we needed buy-in from busy, skeptical hospital physicians. The absence of such documents made it more challenging to advocate for my friend and undermined his case.

Amber proposes ways to bridge the divide between the medical establishment and the ME/CFS world.
Put yourself in the shoes of a busy (and doubtful) emergency room doctor or hospitalist. They do not have time to digest the latest peer-reviewed research on ME/CFS and likely have negative biases about the disease. After the hospital finally released Theo, two papers came out – an article from the UK on life-threatening malnutrition and a published account by a person with very severe ME/CFS. These resources would have been beneficial for Theo’s case. Severe malnutrition is not uncommon in people with very severe ME/CFS.
In the absence of accurate information about very severe ME/CFS, many physicians conclude a malnourished patient must have an eating disorder and, therefore, a psychiatric condition. We need to change this narrative.
The US ME/CFS Clinician Coalition has excellent summary documents for physicians (their most recent documents on testing and treatment came out after Theo left the hospital). However, these statements are geared toward the moderate or moderate-severe portion of the spectrum and do not cover severe malnutrition and its possible causes.
The CDC has vastly improved its website in recent years. However, it still trivializes those severely affected with ME/CFS, offering lifestyle suggestions and recommending therapy. There is no mention of severe malnutrition and how it is commonly mistaken for an eating disorder. The CDC’s recommendations validate false stereotypes about the disease, especially when viewed through the lens of a doubtful doctor. We decided this information would do more harm than good to Theo and chose not to share it.
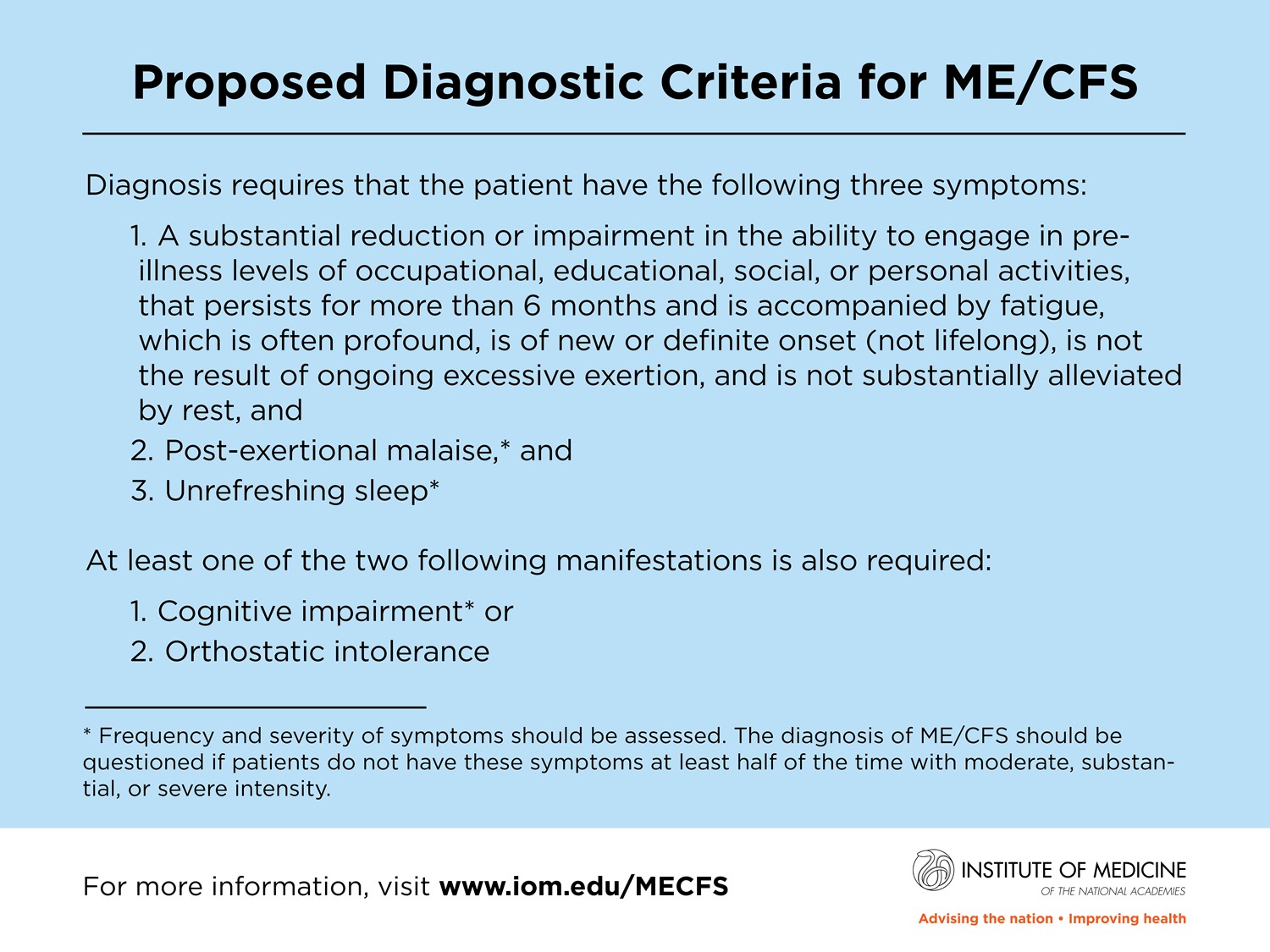
We need statements that capture the entire range of the disease spectrum. The current diagnostic criteria for ME/CFS do not address the most vexing problems that people with very severe illness face – malnutrition and sensory issues. The IOM criteria include the following: fatigue not alleviated by rest and the associated impairment in function, post-exertional malaise, unrefreshing sleep, cognitive impairment, or orthostatic intolerance.
There is nothing about malnutrition and its drivers on this list. While people with very severe ME/CFS experience all of these symptoms, life-threatening malnutrition and severe reactions to food and medications are often the top priorities.
I encourage the Clinician Coalition to consider the needs of those very severely affected by the disease, including a concise document for general practice doctors and hospital staff who have no experience working with this type of patient. Ideally, this document would discuss the unique medical conditions common to people with very severe ME/CFS.
We also need a document that provides a differential diagnosis blueprint for ME/CFS patients experiencing severe malnutrition. Some likely culprits driving weight loss, food intolerances, and GI dysfunction include gastroparesis, delayed motility in the small intestine, malabsorption, abdominal vascular compression syndromes, small intestinal bacterial overgrowth (SIBO), spinal abnormalities, mast cell disease, and more. These are somewhat rare, poorly understood conditions that require specialized diagnostic tests and treatments.
While Theo was in the hospital, the psychiatric team trotted out graded exercise and talk therapy treatments. These therapies have no support in the medical literature as viable treatments for ME/CFS, yet this mentality persists in hospitals and doctors’ offices. Speaking comes at a high cost, and exercise is out of the question in very severe ME/CFS. Refusing this type of treatment only worsens the situation and feeds the psychiatric narrative about the disease, placing patients in a tough spot.
The official materials on exercise intolerance are vague and confusing, despite impairments in energy metabolism being a core feature of ME/CFS. The proposed disease name – systemic exertion intolerance disease (SEID) – is a name that never took hold. Most doctors have no clue what post-exertional malaise is.
Malaise is an unfortunate term because it feeds the psychiatric narrative about the disease. The definition for malaise is “a general feeling of discomfort, illness, or uneasiness whose exact cause is difficult to identify.” Yet we do know enough about the cause of PEM – it is time to call it what it is – lowered functional capacity due to dysfunction in aerobic energy metabolism. Even cognitive tasks, such as thinking and speaking, use oxidative energy metabolism. We need to convey that exposure to light and sounds are like exercise for people with very severe ME/CFS, sometimes causing permanent crashes and further loss of function.

“Having the right resources promptly could make the difference between bringing a patient home vs. placing them in a psychiatric institution.”
We could not find an official source (e.g., Clinician Coalition, CDC) that explicitly states that aerobic activities are contraindicated, especially on the severe end of the spectrum. Exercise and ME/CFS are nuanced topics, but most physicians lack time to digest the literature on why aerobic activities are risky. Thankfully, Workwell Foundation has a powerful letter for physicians that explains why people with ME/CFS have exercise intolerance and caution against aerobic exercise.
We need a packet of materials that people can easily access when a very severe ME/CFS patient is held against their will or is refused treatment by hospitals. This situation is a very traumatic and chaotic experience, and time is critical in a civil commitment case. Having the right resources promptly could make the difference between bringing a patient home vs. placing them in a psychiatric institution.
-
No general contractor
Those with very severe illness cannot travel for medical care, and very few have an ME/CFS specialist. Many people even struggle to find a helpful general practice doctor (GP). Given that GPs are the most likely physicians to interact with very severe ME/CFS patients, we need to invest more in building capacity in primary care.
Being a general contractor is not in the wheelhouse of a busy general practice doctor, yet people with very severe ME/CFS need one. When a medical issue gets elevated beyond the purview of a GP, they typically refer patients to specialists. While this may work for some conditions, those with a complex multisystem illness end up on a conveyor belt of fragmented medical care that yields little insight. Specialists seen in isolation run their standard tests, many of which routinely come up negative. These patients require an integrated care model in which there is cross-talk among specialties.
Over time, very severe patients have less access to primary medical care simply because they become too sick to manage their cases. Many GPs don’t want to take on a highly complex patient or know how to handle one. These patients end up falling through the cracks, have no meaningful medical care, and continue to waste away in isolation.
In the Dialogues of a Forgotten Illness series on severe and very severe ME/CFS, Nigel Speight, M.D., discusses the need for a particular type of GP that harkens back days long gone. People with severe ME/CFS need GPs who can make house calls and coordinate among the various specialists involved with a complex patient. We also need GPs who understand the emotional experience of severely ill patients and how isolation, neglect, abuse, poverty, gaslighting, and medical trauma take their toll on well-being.
Most GPs lack time to devote to understanding the intricacies of ME/CFS, but the Bateman Horne Center and the Clinician Coalition offer models for educating physicians. Dr. Bateman’s passion for building capacity in GPs has already built capacity in some regions. Similarly, some ME/CFS organizations have developed online continuing medical education courses. While these are excellent resources, we also need funding for a fellowship program pairing physicians and physician assistants with ME/CFS clinicians. Such a program would help address the shortage of ME/CFS-literate physicians throughout the United States (and beyond).
After the hospital debacle, Theo and I had the good fortune of finding a new GP who shadowed Dr. Bateman. Theo’s new doctor allows complex patients to schedule extended consultations, makes video appointments, and participates in peer-to-peer consultations with experts in the various co-morbidities associated with ME/CFS. We need more GPs like her.
-
Lack of savvy medical advocates
Very severe patients cannot manage their activities of daily living, doctors’ appointments, prescriptions, home health, nursing, and other services. They need a medical advocate who is somewhat knowledgeable about ME/CFS and can ensure patients meet their goals.
An advocate must convey subtleties of the patient’s experience and be conversant in medicine and pharmacology related to the disease (but need not have a medical background, just a keen interest). An advocate is also important for ensuring follow-through on prescriptions and referrals, coordinating caregivers, implementing treatment plans, and, in general, working through any problems that arise.

An ME Buddy system could help keep the very severely ill from tumbling over the brink.
We need an ME buddy system. Medical advocates from agencies can be prohibitively expensive and likely have no experience with ME/CS, potentially introducing more harm. A formal buddy system pairing a family member, friend, or fellow person with ME/CFS who can commit would be ideal. People with severe ME/CFS have diverse needs, including legal, medical, fundraising needs, emotional support, logistics (transport, errands), and more. It would be unreasonable for one person to do all of these tasks, but help with any of them could be meaningful to a person with very severe ME/CFS. Medical advocates can do much of this work from afar. It is essential for people serving in this role to be clear on what the patient can expect.
-
Legal roadblocks
A few years ago, I tried to advocate for another friend with very severe ME/CFS but felt helpless as I watched her slip away from afar. I spent many hours attempting to connect her reluctant GP with ME/CFS clinicians and other specialists for peer-to-peer consultations. These efforts rarely went anywhere or took far too long to be meaningful. I could not find an ME/CFS clinician who would take her on as a patient because she could not travel to see them (state laws require many doctors to see patients in person). It was deeply frustrating to feel so ineffective while knowing what could help my friend.
Ultimately, she approached the line in the sand for many severely ill patients, maintaining her agency. In the end, she took her life because she saw no way out and did not want to end up in an institution where she would have little control over her life. I vowed I would never let that happen again to a friend.
While Theo was in the hospital, I became his medical power of attorney (POA), but this took time to set up and was challenging to execute in a hospital during COVID. Being POA has allowed me to cut through layers of bureaucracy and speak to doctors and lawyers on Theo’s behalf.
The designated POA must be committed to representing the patient’s interests. Being POA is a significant responsibility, and whoever fills this role must be trustworthy and up for the task. Ideally, a family member could serve in this capacity, but many patients do not have supportive families. For a list of medical power of attorney forms by state, click here.
It is hard to summarize the legal issues facing patients because each state has different laws. However, we need a document that provides general guidance on the types of legal roadblocks that arise when hospitals deny patients treatment or hold them against their will.
-
Lack of family support, or worse
Over the years, as routine tests come back negative, doubts can begin to set in with families. Misinformed doctors and society amplify this message. As a family member becomes sicker, they become more of a burden. Even loving families can begin to convince themselves that it might be best to institutionalize their sick loved one.
People with very severe ME/CFS need sustained validation and support from their families and friends.
-
Poverty
Poverty undermines the health and well-being of very severe patients. This situation applies to all people with ME/CFS who cannot work but is even more devastating for very severely ill patients, especially those on Supplemental Security Income (SSI). This program requires you to be poor and stay poor.
Most ME/CFS specialists have private practices that can cost hundreds, if not thousands of dollars per hour. Disabled patients cannot afford these rates and are at the mercy of their local GP.
People with very severe ME/CFS often need fundraisers to help cover the expenses of medications, supplements, private testing, and specialists. Many of these patients are on SSDI or SSI and receive benefits from other means-tested programs. GoFundMe accounts, Paypal donations, etc., are considered deductible income, putting benefits, and the limited life-line patients have at risk. Losing benefits and reapplying could be devastating for a very severely ill person who is barely hanging on.
Fundraising under an emergency, such as when hospitals hold patients against their will, further exacerbates this problem. State laws around this subject are complex. Even well-meaning friends and family could undermine people with very severe illness in the heat of a crisis. Friends and family need to think through the financial ramifications of additional income, especially for means-tested programs.
Consider consulting with an attorney on trusts or opening an Achieving a Better Life (ABLE) Act account, a program for those who became ill on or before age 26. This program allows people on SSI to have savings accounts for medical purposes. We opted for the latter in Theo’s case because he qualified for the ABLE program. Understanding what is permissible is essential before transferring GoFundMe or similar funds to a bank account.
Next steps

Amber’s assertion: we can do better to support the very severely ill.
We need to move beyond the chaos of the case-by-case approach when hospitals threaten very severe ME/CFS patients with involuntary commitment, graded exercise, and talk therapy. Currently, no organization specializes in helping patients and families through acute crises like my friend Theo experienced. Each time this occurs, we need to reinvent the wheel, costing patients precious time and health.
The following actions would be a step in the right direction:
-
- Include people with very severe ME/CFS as primary stakeholders. We need to find ways to have their ideas heard.
- Develop a concise and authoritative document for medical staff about the unique medical needs of people with very severe ME/CFS, emphasizing gastrointestinal manifestations and extreme sensitivities to food, medications, sound, light, and more. Ideally, this document would list possible causes of weight loss and malnutrition and offer potential treatment solutions. We need a document that unequivocally states why aerobic exercise and activity are contraindicated.
- Update CDC website to state that aerobic exercise and activity is contraindicated in ME/CFS, especially on the severe end of the spectrum.
- Develop a training program for general practice doctors. Ideally, the program would enlist at least one physician from each state in the US. This program could involve shadowing ME/CFS clinicians at their clinics. This approach would offer a quick way to build capacity in primary care.
- Develop a ME/CFS buddy system program. This program would take some thought to get right and involve training friends, family members, and people with ME/CFS to be a medical advocate for someone with very severe ME/CFS.
- Designate a trusted person to serve as power of attorney.
- Consider setting up a trust or ABLE account for those eligible to build financial resiliency.
Most of all, people with very severe ME/CFS need love, support, and validation from the people in their lives. Ignoring people or hoping the problem will go away will only push them deeper into their illness, sometimes beyond the point of no return.
______________________________________________________________________
Concise and authoritative resources on the diagnosis and treatment of ME/CFS that could be helpful when advocating for a person with very severe ME/CFS
This list below is not exhaustive but instead focuses on statements that offer concise and authoritative sources written by physicians for physicians. There are much longer reports and books available, but these are unlikely to be helpful in the heat of the moment when patients encounter doubtful hospital personnel.
Baxter, H, N Speight, W. Weir. 2021. Life-threatening malnutrition in very severe ME/CFS. Healthcare 9: 459. Not concise, but this is an excellent resource that describes how malnourished patients are wrongly diagnosed with psychiatric illnesses.
IOM/National Academy of Medicine Report – Redefining an Illness:
Report Guide for Clinicians (2015) No mention of malnutrition and vague on exercise intolerance.
Diagnosing and treating myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) – US ME/CFS Clinician Coalition (2020) An excellent resource but does not address the very severe end of the disease spectrum.
Testing recommendations for suspected ME/CFS Version 1 – US ME/CFS Clinician Coalition (2021) Excellent but incomplete for a differential diagnosis for malnutrition.
ME/CFS Treatment Recommendations Version1 – US ME/CFS Clinician Coalition (2021) Excellent resource offers many treatment ideas that could help a person with very severe ME/CFS but falls short on treatments for gastrointestinal manifestations of the disease.
https://workwellfoundation.org/wp-content/uploads/2019/07/MECFS-GET-Letter-to-Health-Care-Providers-v4-30-2.pdf This is an excellent resource to provide to physicians struggling to understand exercise intolerance.
Komaroff, AL. 2019. Advances in Understanding the Pathophysiology of Chronic Fatigue Syndrome. JAMA. 322 (6): 499-500 (2-page paper behind paywall)



{kind=link}
This is simply excellent.
And terrifying.
Well said. And thanks Amber for caring and acting on behalf of the worst of patients and trying to improve things for them. It is much appreciated.
Lovely article! So wish there was more people like you in the world. Caring for others and with a heart of gold…..the one thing of most value is our time. That doesn’t cost money, but its our most valued possession…..we don’t get that back. It takes a heart like yours to care and put themselves out for someone else who desperately needs help. Thank you Amber on behalf of those who your kindness has helped. Well done! I hope that others will be able to see the need, and if their hearts motivate them, they will come to the aid of others in such kind acts of “being there” when they are in such great need. Thanks for being such a fine example and advocate!
Thank you, dejurgen, for your kind comments. I am hoping we can put some of the ideas in the piece into action.
https://www.youtube.com/watch?v=4LX_JRHZdkI
Thank you!
I am to ill to read it. only a few sentences in the beginning. thank you cort!!!
thank you for writing about us!!!
I hope i can read and response another time.
After 2 vaccines even worse, live alone, bad not educated helpservice who is unhygienic, the princes downstairs (I lay in bed), wears no mask, i get not washed, etc
do not know what to do anymore, where to “go”.
here in belgium it is still get and cbt, ME does not excists, cfs doe, with a couple of seessions cbt and get. to ill for oldmanshome, to ill for even psychiatry, to ill for anything
wish it was over. not that i do not want to live, i want to live so much, but there is for me no future, only decline and more suffering and that i do not want.
long forgotten, rotting in hell… gp does know nothing, even no symptomtratments, threatening me to put me away, oh so much, i had it all…
Thanks Konjin for Amber who wrote this wonderful piece – a foundational document really which will – if we take up the challenge – change people’s lives.
Het spijt me zo dat je op zo’n moeilijke plek bent! Ik woonde een tijdje uit in België. Je bent in mijn gebeden konijn
Konjin – my heart goes out to you. It is shameful that people like you are slipping through the cracks and landing in a place with no meaningful help. I dearly wish we had residential places where we could receive appropriate care. It shouldn’t be this hard. Please know that I am thinking of you – you are not forgotten. Even in your much-diminished state of health, you bring so much to this forum and are a valued member of our community. Sending very best thoughts your way.
may i if i can, put your article in 25%ME fb site?
I would be happy to have you share the piece any place you would like. Thank you for helping to get the word out!
when i saw once a picture of whithney, it shocked me how clean he was and how clean it was there. but he has parents who take care of him. luckily!
there should have been long time adapted homes for those who are alone or mistreated or anything. like for MS patiets.
For Konijn: My heart goes out to you, Konijn, and all others in similar situations. Those without supportive family and adequate funds/insurance and even basic civil rights at this point are the worst off of all those with ME/CFS. Those unable to communicate powerfully, skillfully, charmingly with the med heads are often misunderstood, imprisoned and medicated with unnecessary poisons by a greedy psych industry to the point of inspiring the experiencer to leave the planet.
No financially well off person in my experience has ever been able to grasp these complex long term situations except the most rare and superconscious ME counselors and physicians (who I will not name here) or can begin to imagine the despairing hardship that comes with not being able to afford the right types of help. Optimism, persistence and “positive thinking” cannot do it all for those without enough safety net.
You are understood and accepted here, Konijn.
I pray that some angelic-type person will advocate for you successfully, permanently.
I have not had the resources to help others as I strongly choose. Sometimes just an encouraging kind word to someone unrelated to ME/CFS will be at least a ripple of goodness in the universe that somehow may end up assisting you in some surprise way, I hope. This is an intention that the so-called Butterfly Effect is for real, and for good. More revelations from quantum physics may one day prove this beyond all doubt.
Amber Ella is another hero in this sphere. You are extremely articulate about our needs, Amber; thanks also to those who add to the forward movement here. I will keep her and this advocacy project in my daily energy intentions. And Cort as always. All of us too!
Becca – thank you for your powerful words and thoughts. I really hope we can all come together and pick up on some of these threads to improve the lives of people like Konjin, who suffer immensely. I will be devoting more energy to this project in the coming months and appreciate all of the heartfelt thoughts and ideas everyone is sharing. Thank you.
Excellent article! I hope someone is able to enact your recommendations and get the changes made to the CDC website etc.
When we remember the severity of our disease, so many of us must just be so grateful that we are not so sick.
I just wish we would stop referring to doctors like Teitelbaum and Myhill as “experts.”
Doctors that do at least have some understanding of our disease need to band together and pressure Congress for action, as was done back in the AIDS era.
If I could I would definitely create a safe supportive place for severe me patients. I relate to what you are saying konijn. Especially today.
Thank you, Gregory. I agree – the CDC website needs some serious help. Initially, I was happy to see the revamp they did a couple of years ago, but in our time of need, when my friend was being held against his will in the hospital, I realized how bad the CDC site on severe ME is. Their guidance for the sickest of the sick amounts to talk therapy, PT, pacing, and lifestyle advice.
Here is one not so helpful quote: “For example, they can consider sitting instead of standing when cooking or showering, using a bedside commode in lieu of walking to the restroom, and taking frequent breaks during activity.” WTH? Nothing about comorbidities driving very severe ME. Nothing about a differential diagnosis. Certainly nothing about weight loss, intolerance to foods and medications, and malnutrition and its drivers. This feeds the biopsychosocial narrative.
But it isn’t just the CDC. Many of the ME organizations do a somewhat good job providing information on moderate/moderate-severe ME. However, it seems as if there is a point at which the advice goes from meaningful to harmful as the severity level increases. The people who need the most medical care end up getting the least and are told to think good thoughts, pace, and try to do some movement.
I think the following is from a further update on the CDC site. Maybe it was because of your efforts:
“Any activity or exercise plan for people with ME/CFS needs to be carefully designed with input from each patient. While vigorous aerobic exercise can be beneficial for many chronic illnesses, patients with ME/CFS do not tolerate such exercise routines. Standard exercise recommendations for healthy people can be harmful for patients with ME/CFS. However, it is important that patients with ME/CFS undertake activities that they can tolerate, as described above.”
It is found here: https://www.cdc.gov/me-cfs/treatment/index.html
Excellent article……the only thing I’d add is that many of these recommendations actually apply when one is moderately ill; not just very severely ill (& if they were put into place & made known as issues that can arise when one is moderately ill, they could help prevent many from reaching the pt of severely or very severely ill). This is esp the case when someone who is moderately ill has absolutely no practical help for ADLs, etc, so no chance to pace many things that life throws at them, & no one who can advocate for their needs, or back them up when they do try to explain their own needs, etc.
I am currently severely ill, but I have had the motility & nutrition issues, the sensory issues, the severe reactions due to mast cell & MCS & allergies, etc….have had problems interacting with anyone on the phone, on video, or in person, etc, etc, …have had several of the issues that are brought up here as applying to the very severely ill & some other ones, as well (but it sounds to me like this is saying they only apply to the very severely ill)…..but I have had those issues since I was moderate.
They have just continued to get worse as I’ve become more ill, because back when I was moderate & actually stood a chance of having any help, no one would listen or believe me about that stuff. So, I was forced into consistently overdoing it, not being able to get help re my nutrition issues, my mast cell reactions, my sensory issues, etc, etc, or any of my ADL.s, or other random things that life brings up that have to be taken care of……..& as a result I continued to decline……I am now past that pt of return myself – not in a suicidal way (my faith prevents that, thankfully), but in that I am literally too sick to even handle having any help anymore.
I could not stand to have anyone even in my apt with me, let alone have them actively doing the thigns I need, nor would I be able to explain those needs to them, or what constitutes being truly fragrance free, etc, etc….am unable to travel for treatment (even 10 mins is too far), etc, etc. I definitely can’t afford help either….and the issues with being unable to get help go on & on.
And, while the article brought up the issues with regards to fund raisers potentially causing more problems, & I’m glad it did, bc far too many people are unaware of that stuff, & the system itself is stacked against those of us who are very poor & very ill, there are also many major issues simply with getting the govt help that is in place (& many of those issues vary depending on the state one lives in, too)…..and there are even more huge issues with continuing to prove disability. (I am seriously way too sick to even prove that I am this sick anymore. If I ever have to got thru another long form cont dis proof, I am pretty much screwed. I did have to go thru it one time back when I was moderate, & it left me permanently much sicker. It was actually harder than the initial proof…….& most know how incredibly hard that is!) There is something very wrong with a system that makes it possible for someone to be too sick to prove they are sick!
Another thing that really needs something done abotu it is the fund that was mentioned for those who become ill prior to turning 26. While it is a great help to those who did so, there are so many of us who fall thru those cracks, too, becasue we got sick at somewhere in between 26 & retirement age.
None of this is a criticism of the article at all. I am happy to see it written, & agree very much with what was said. And, I don’t have solutions for any of what I brought up. I just feel that it is important to note that it’s not just the very severely ill who are falling between the cracks & being failed……many of these issues apply to those who are moderately ill & totally without help &/or have multiple co-morbidities. And, if they could be addressed sooner, than maybe fewer would be failed.
thank you aunt tammie
I can so very much relate ..I appreciate your advocacy for us in the “moderate” and over 26 become ill catagory.. I was probably hit withy my first bout of illness in very early 20s but nothing is/was documented.. am now 54.. and been seeing a steadly decline sometimes the decline is sharp. 🙁 and I struggle to keep up with my bodies basic needs and my apartment is a mess.. live becomes small..I have finally gotten ok with that. ..after 20 years. I am not able to get IHHS because I dont quailfy for Medi-cal.. even If i did i have heard it is hard to get helpers esp since covid..and even before covid the cost of living in the bay area is more than many Home health helpers can afford. I appreciate all the help and info here. thank you
Qualification for the ABLE investment fund can possibly be done if there are even any very old medical records, family correspondence among family members or with doctors, insurance, guidance counselors notes, employment records, personal journaling, etc. about any type of disability before age 26. Good listmaking helps. Lie in bed, think and see what surfaces.
I know because I did it. There is some leeway. Maybe the laws will change more now in people’s favor.
Qualification for the ABLE investment fund can possibly be done if there are even any very old medical records, family correspondence among family members or with doctors, insurance, guidance counselors notes, employment records, personal journaling, etc. about any type of disability before age 26. Good list making helps. Lie in bed, think and see what surfaces.
I know because I did it. There is some leeway. Maybe the laws will change more now in people’s favor.
I agree with everyone you say above. I tried to make a similar point – that we need to catch people before they fall into the spiral downward. I would like to believe that if we understand the underlying processes that lead someone to the place of very severe ME, we could get better at spotting comorbidities in their early stages before they progress to the point of no return. As you say, many of these conditions affect moderately ill people, including mast cell disease, gastroparesis, SIBO, compression syndromes, etc. Sadly, sometimes these conditions are caught too late.
Perhaps there would be value in doing a case history-type approach with those who have become severely and very severely affected. What were the first warning signs to indicate the downward spiral? I also think it would be helpful to learn more about how social structures (family, friends, GP, local hospitals, etc.) break down along the way.
This so so resonates with me and my experience of having a daughter with severe ME/CFS in hospital, I was blamed for making her ill, I had to listen to the “mind/body” banter. My son and I tag teamed sleeping in her bathroom as the nurses bullied her less if we were around. The general physician threatened our GP with a malpractice suit for “supporting” us to refuse GET/CBT on the basis of the PACE trial results. Fortunately after reading an article that we had found by Nancy Klimas, about the harms of GET the physio’s refused to “rehabilitate” my daughter. They could see that she looked skeltal and suggeted that she was secretly getting out of bed to vomit. We were lucky that a GP friend talked to the first treating physician and before he handed the case over to his colleague, he wrote detailed case notes to “save her” from mental health brigade. Our most critical need was and still is for authoritarian resources about hypersensitivity to : food, noise, light and chemical intolerance.
I am so sorry you and your daughter suffered this abuse and disbelief. You touch on a topic I did not cover in my piece – minors who are severely ill. As parents, we walk a fine line when advocating for our children. It is horrifying enough when an adult is held against their will, but having a child taken from you simply for trying to get them the care they need is terrifying. We have seen so many of these stories play out over the years. I am so glad you made it out of that situation.
In my case food intolerances were the direct cause of becomming underweight. I was down to eating one Meals on Wheels meal a day when my dietician said that I was eating so little and not hungry because my body was intolerant to the food I was trying to eat and therefore rejecting it. My dietician urged me to follow the diet recommendations in the Royal Prince Alfred Elimination Diet from the University of Sydney – https://www.slhd.nsw.gov.au/rpa/allergy/resources/foodintol/ffintro.html. I had a woman cook and freeze basic food as per the strict version of this diet and imediately I ate and ate and ate and ate. I rapidly gained 10 kg and was slightly over my “normal” weight before my appetite slowed and I stopped eating so so much. I am stunned that more than a decade after this receipe and guide to identifying food intolerances has been written and used throughout Australia it is still NOT in the ME/CFS resource kits and not even mentioned in much of the ME/CFS support literature.
Thank you so much for advocating for us xx Here in Australia the NHS won’t even recognize me/cfs. We get no support at all. I am bedbound 24/7 and have been through hell with the medical system. My local Doctor Dr. Davey in Lobethal refuses to home visit me, even though he does do home visits 🙁 I have been mocked and ridiculed by the receptionist at that practice as well. When I go to ER I have to explain what me/cfs is and as soon as I mention the word Chronic Fatigue, eyebrows get raised and I am sent on my way “sorry nothing we can do for you” So I am left to rot in my bed at home 24/7. Thank goodness, my husband is my carer otherwise it would be a nursing home for me, where it would be a nightmare. I have showered twice in 5 months as taking a shower exhausts me. I have to sit on a chair in the shower.
It boggles the mind how some of the best research on ME comes out of Australia, yet you are in the dark ages when it comes to ME care.
I wish care facilities were a more viable option – but we know that so much more harm can be done if people have the wrong idea about what makes us sick. So glad you have your husband to help with your care.
Wow Amber. Astounding. You’ve really hit it out of the ball park with this.
If you can get any momentum behind even a fraction of what you’re proposing here, you’ll have accomplished more *practical* help for ME/CFS patients than I’ve seen in my entire lifetime.
As someone who is housebound, and often bedbound, I applaud you for raising this issue, and recognizing that virtually all of the descriptions re: ‘help’ for ME/CFS patients are for the lightly or at most moderately ill. At this stage of my life I rarely ever try to access medical care, because the (former) constant parade of doctors who at best give you the ‘blink-blink’ response, but who most often give you the equivalent of raised crosses and garlic when you attempt to see them comes at too high a price. And that price often includes not just a brush off, but too often actual threat to our well-being from our medical providers. It’s like we’re still in the middle ages here, where your surgeon is more likely to maim or kill you as s/he is to help you heal.
You’ve identified SO many of the unknown, unaddressed &/or un-acknowledged needs, in such a methodical way, that I have to say you have a real skill at this. I’m only sorry (very, very sorry) that so much of your knowledge was acquired through the death of your friend.
Bless you for what you’ve done, and what you’re doing.
Your analogy to the early days of surgery seems so apt here. The abuse, derision, conceit, and callousness toward extremely ill people should belong to the late 19th century. Yet here we are.
My efforts in the coming months will be to work with those with authority to provide an emergency packet for patients and families who are being threatened, as many dear friends have experienced. It would be a starting point. But there is so much to do – and it will take a group of committed and dedicated people to see some of these ideas come to fruition.
I think this is such vital information Amber. ‘We need a packet of materials that people can easily access when a very severe ME/CFS patient is held against their will or is refused treatment by hospitals.’ Seems to me to be such a sensible common sense approach and could avoid losing time, searching for relevant information, in a time critical situation. So well put together. Yes!
Thank you!
This guy on TV,(US) not one of us, but he did have two cancers after his GP said don’t worry about it. When asked on the Doctor Oz show, “What was your greatest difficulty” his reply,
” The Total Lack of Understanding.”
Thank you Amber for writing this article. I live in the U.K. and my ME is severe, I am bedbound and have sensitivities. I have given up with doctors because I cannot find one who will listen to what I try to tell them about my condition. In the beginning I had one good doctor who would listen but she left the practice. Even so she did not understand the illness, I was mild at that time and she did often ask me if I was depressed which seems to be a common theme with doctors. At the moment my elderly husband cares for me but should something happen to him I will end up in care. This is a scenario that I dread as I am sure that this would cause me to deteriorate even further due to lack of understanding of my needs. I wholeheartedly agree that there is a desperate need to bring awareness to the medical profession of the needs of people with ME at all levels to prevent their deterioration but certainly a heightened awareness of those that have already become far too ill to advocate for themselves.
I feel what you are saying. I have many friends with aging caregivers and are wondering what the future will look like. There is not much of a safety net for us – but how can we build more resiliency?
Perhaps it would help if we had more GPs and ME clinicians who treat this is the progressive condition it is for many of us. I know this disease manifests in diverse ways, but I am guessing there are patterns to decline over time. Imagine having GP who could give us some straight talk and say, “well, you have a progressive disease. Here are the things we will be watching out for, and here is what we will do if they arise. Many of the co-morbidities have no cure, but we can try to slow the progression and manage symptoms.” I know, I am speaking about unicorns here.
I thought that perhaps the growing body of scientific research from recent years might be starting to turn the tide for patients but this illness is still very much a human rights issue. So many of us face closed doors and closed minds at every turn. Thank you Amber for your valuable efforts to change things for the most vulnerable amongst us who deserve so much better.
Exactly, debsw! This has long been a civil and human rights issue worldwide. Who remembers in the 1980s how the AIDS folks, mostly male, intensely networked and demonstrated? They kept at it. After a time many got what they needed to prevail, be independent and thrive in life. I think there was an international group called Act Up.
A few years ago some people in this forum cautioned everybody with ME/CFIDS issues when addressing authorities for lack of funds and action to “be polite, nice, you will catch more flies with honey than vinegar,” that kind of non-assertive approach. Assertiveness is not aggressiveness; it is effectiveness. What did polite pleading get anyone with AIDS?
Activist skill needs only to be effective in getting ME/CFIDS civil and human rights met worldwide. Those denying us these basic rights need to be called on the carpet and their negligence exposed fast, exactly what the fatigued activists here and many other forums are doing.
Follow and expose the money trail when basic rights of are denied. I think this truly is a civil rights issue and should among other great actions like Amber’s be addressed as such with powerful attorneys who speak for the crushed like Daniel Sheehan or Erin Brockovitch. Too many of those who ask hard questions have been intentionally suppressed. Those who make huge salaries and switch from job to job in corporate/governmental disease management bureaucracies for forty years or so are in no hurry to give up their power, lifestyles and ignorance. Forty or more years and still doctors/administrators worldwide are ignorant of how to truly heal or give basic respect, services and compassion to those suffering from these neuroimmune diseases disabling millions, most of whom are women? That did not happen by accident or lack of good data for that long.
Powerful info packets might include an overview on timelines re: how bureaucracies have mishandled these issues. –And tips on the most productive advocacy skills.
Every power broker in the world has an army of strong assistants to carry out a single agenda.
We deserve no less.
Thank you Amber. Obviously your article resonates with all of us no matter what stage of illness we are suffering. Moderate leading to severe because much of it is attributed mistakenly to our “mental health” which actually declines due to chronic illness itself! I used to be a gym rat and avid hiker and did yoga daily at home and that was excellent for mental and physical health. Now I can’t do any of that and I live in a state of GRIEF for the physical losses I’ve been facing. Of course it’s depressing! And of course anxiety about continuing to worsen physically is present as we start to feel helpless about just the very basic human needs to survive! Being “misunderstood” and “not taken seriously” are the norm. God bless each and every one of us and make ways where there seem to be none.
Thank you, Mary. It seems we acquire more and more trauma the longer we are at this. It causes me great pain to think of so many desperately ill people seeking help and being met with nothing but callousness.
Exactly. Thank YOU Amber! You are obviously a very empathetic and passionate advocate for all of us. What a SWEET HEART you have !
It was heartbreaking and frightening to read the stories of those with the severest ME/CFS. Frightening because we all may just be a year or two away from this degree of illness,
The problem we have is the government’s refusal to give more than lip service to ME/CFS. This trivializes the illness which carries over to uninformed medical professionals that is until they have ME/CFS themselves. I have had two doctors who fall into this category.
There are, however, two solid areas of confirmation of the reality of ME/CFS. 1) you cannot donate blood if you have ME/CFS 2) you cannot buy long term care insurance.
The AABB, an organization representing blood banking centers in the United States and around the world, has recommended the indefinite deferral of potential blood donors with a past or current history of ME/CFS. This recommendation has been adopted by the American Red Cross and America’s Blood Centers, the two largest blood collectors in the United States.
My husband and I were also shocked when I was turned down for long term care insurance because of my diagnosis. We had recently cared for two sets of elderly parents and knew how expensive assisted living care could be.
But, the insurance industry knows….they always know.
Betty, I’m so sorry, but not surprised, you were turned down for long term care insurance. Had you any inkling of this before it happened?
I’ve long thought that the most effective ME/CFS awareness effort would be to pick a day and get as many of us as could drag ourselves out of the bed or house (world-wide!!!) to queue up in front of blood donation centres and hand out three pieces of information to passers-by:
1) the published research showing that healthy red blood cells become deformed when in our plasma:
– showing that if we were to donate blood this would injure the recipient’s blood cells
2) studies showing how long it takes on average to get an ME/CFS diagnosis:
– highlighting the overwhelmingly discredited (but yet still rampantly endorsed) bad science labelling this as psychosomatic despite many studies documenting the serious health implications, and despite blood banks disallowing donation, and insurance companies denying coverage;
– highlighting the profound lack of treatment providers who can give a valid diagnosis;
– with the clear implication that the blood of as yet undiagnosed ME/CFS patients may already (unknowingly) be in the blood supply
3) documentation about the disease burden and complete lack of treatment for ME/CFS in relation to its funding:
– implying that this is the public’s possible fate should they develop this disease, whether via blood transfusion or otherwise.
If we want the public to take an interest and help us drive change, we need to make it personal to them. And this is a valid concern that I don’t see anyone talking about, but should make the average person nervous.
There are so many arresting visual aids that could be used: a few of us in line carrying IV poles with (fake) blood with big ‘Poison’ stickers on it, for instance, would instantly convey an image that’s hard to forget. Or carrying signs saying “Health care policy says our disease is psychosomatic, so WE DEMAND THE RIGHT TO DONATE BLOOD!” Etc…
This is just me venting (not a real suggestion, but after 40 years of nothing but prejudice and promised funds being ‘woops’ directed elsewhere, perhaps it’s not so outlandish an idea…) If we’re ever at the point of considering guerrilla tactics we could all arrange to quietly queue up to donate blood (WORLD WIDE!) on the same day, and then ‘woops’ disclose just before they start to draw it that we have ME/CFS. With enough people doing this across multiple locations/countries, and enough journalists onboard equipped with a few judiciously worded press releases to go alongside, I’m sure we could finally get some press to pushback against the ‘this is all in your head’ narrative that’s been following us like stinky cheese since forever, and ask why we’re still in this position after 40 years(!!!) of inaction.
I really liked your ideas.
Thanks, Cort, for bringing attention to severe ME/CFS with these last two articles. This is a very neglected area, even within the almost total neglect of ME/CFS by medical ‘authorities’. These observations help give voice to this population, even if what they have to say is dark. Hard truths need to be spoken about this disease and the extreme stigmatization of it (and the patients who suffer) if we’re ever to start to see the light.
I hope these stories will help serve as a caution to those with moderate illness to take their health boundaries seriously so as to avoid crashing further, and to guard their health jealously.
(Cort, is there *anything* that can be done about the on-going moderation? It’s been months now.)
Thank you for thanking me for publishing Amber’s call for more resources for the severely ill. All of her suggestions are doable and some of them are pretty easily doable. I hope her paper will elicit more discussion and more importantly action to support the very severely ill.
As to the wonky moderation – I’m sorry but I just have no idea how to improve it. It does very well to screen out literally thousands of spam attempts but gets things wrong at time – and puts commenters – including some of our most prolific commenters into the queue when they shouldn’t be.
‘
My thanks was far too tepid. Thank you sincerely Cort – it’s a very important thing you’re doing here. It’s a great credit to you that you’ve waded into territory few others have dared to tread.
I know it can be very challenging to cover things which are controversial, or liable to arouse strong emotions such as these last two posts. Even more credit to you that you allowed both Whitney and Amber to speak so strongly in their own voice.
I hope you’ll continue to follow up with both of them, and even perhaps work with both of them in the future. I think that would be helpful for so many of us.
These were both very hard-hitting posts, but in my experience this kind of thing (along with your Fauci post) is Health Rising at its best. Thank you.
I agree with you Anne – Thank you, Cort, for providing this venue for us to explore ideas and advocate.
Amber, what is the name and location of the physician who is helping? I think, we as a community should build a data base of helpful medical personnel. How can we do this. My doctor is Dr. James Willoughby, DO in Liberty, Mo. Next, we need the Coalition to put the 2 day CPET test high on their list. Until we get diagnosis, this will all continue. If you prove PEM at the outset, the patient has solid information on self help and the doctor would not have wiggle room on a psychological diagnosis. I plan to gather info from Workwell to take to my community hospital. They need sources of additional income so I am hoping for a financial motive. Additionally, I intend to go to Independence Inc. and begin discussions with them about the support programs Amber is talking about.
I agree that this forum needs to have a serious discussion around foods and gut improvement. I am going to look at the Australian diet mentioned in the comments. I wrote an article on Cort’s request about GAPS plus my thoughts on IgG IgE food testing…not published. I am curious whether any of you has read original work from Dr. Natasha Campbell-McBride, MD, Elaine Gottschall, or The original SCD? We need some more helpful input for the newbies to this site.
Thanks Janet, we need all the people involved we can get. Just an FYI about the histamine/MCAS food lists and diets, they vary greatly and it’s very individual for each person but I found a few helpful lists. This was the first and best , from Switzerland. https://www.histaminintoleranz.ch/en/introduction.html
“Mast Cell 360” Is the best website with food lists and lots of info. https://mastcell360.com/
I would really like to see your article on IgE/IgG because my testing would have alerted me years earlier (along with a prick test that was neg for everything except histamine!) if the DRs new what they were looking at. Please Cort publish her article and give people an early heads up as to what may be coming down the road.
“Please Cort publish her article”
A good start is for one to open a new blog in the comment section and see how much traction it gets. Cort has to take care of his own limited time and energy so selection of what gets priority is his responsibility. We are the visitors benefiting from his efforts. He also is responsible for the content if he publishes it on the main page and has to make sure it meets his standards.
I can’t and wont judge on why something is not published yet, but much can and is published by forum members on the forum so this is an obvious solution for a potential problem.
Thanks Janet, we need all the people involved we can get. Just an FYI about the histamine/MCAS food lists and diets, they vary greatly and it’s very individual for each person but I found a few helpful lists. This was the first and best , from Switzerland. https://www.histaminintoleranz.ch/en/introduction.html
“Mast Cell 360” Is the best website with food lists and lots of info. https://mastcell360.com/
I would really like to see your article on IgE/IgG because my testing would have alerted me years earlier (along with a prick test that was neg for everything except histamine!) if the DRs new what they were looking at. Please Cort, publish her article and give people an early heads up as to what may be coming down the road.
Thanks Amber! This is exactly what we need done to make improvements quickly! I sent a heads up to Solve ME/CFS asking them for their help in putting together forms and documentation which could be part of a packet of documents kept on file by your Dr and in your possession, in case of emergency. My suspicion is that it’s going to take getting attorney’s involved to get Drs to toe the line. This info is a great outline to start from. Thanks!
I was diagnosed 2001 by Dr. Jay Goldstein, another pioneer who saw Epstein-Barr patients originally. His last book Betrayal of the Brain was too technical for me to read. But the title has stayed with me.
I have been involuntarily hospitalized many times. I have a master’s degree in social work, was a Federal Grant writer and became severely ill in the late 1990s. I have followed the research, read every book, joined online support groups. I saw the “experts”. I am attempting to write a blog for Cort. Im so tired of being invisible. Im also weary of fighting this disease totally alone.
Im 63 and while there is our superman, Dr. Ron Davis , out there, it will still be too late for me. I dont have enough money, friends or family support. While they believe my illness now, they cant sacrifice their lives for mine. Nobody understands that I cannot take care of myself and a nursing home is NOT something I will subject myself to. The neuropathy I now have is unbearable. I am burning up.
This is NOT depression. If I was in the last stage of an uncurable cancer, I would have medical support/insurance, hospice, and the right to end my suffering. I am happy with what I accomplished, even though I would like to have done more. Im grateful for the doctors, fellow sufferers for fighting back. Whitney, Jennifer, Laura, Sarah..you are all young with a life ahead of you. I will continue to watch you from my laptop for as long as I can. Life is precious and beautiful. But we all come to a stage where we know it’s been enough. I am smiling.
Susan,
I’ve been pondering end of life options. I’m not in a crisis or critical state ATM, but in a similar state of mind. Many of us long term pwME who are running out of time and options don’t have the same resources as many other folk, as you’ve said. Have you made any preparations–can I ask how have you approached this? Have you gotten legal help for your wishes?
You are not invisible to us Susan.
This illness makes us feel old old old even when we are young. I remember a woman who got better after many years say that she felt better at 65 than 35. I will keep my fingers crossed for you. I hope your neuropathy and extreme suffering ease.
Susan, while my situation is different than yours my feelings are similar. I take huge comfort in your comment–I am not alone! I’m hoping you’ll feel similar if you read this. Good luck to you.
Well Amber, like most everybody else, I’m totally blown away by your article. As AuntTammie said, it also applies to those of us not severely ill.
As I was reading, I realized that it contained, in a narrative kind of way, an outline for setting up a ME/CFS help site where one could find resources for many of the issues you highlighted;
Medical papers to explain to ER or other doctors about our illness–including information about the severely ill and their more unique issues–like malnutrition–not usually mentioned in current literature.
Different diets to deal with many of the food intolerances people experience including information on MCAS, SIBO, IBS and other contributing factors.
Symptom and co-morbidity lists.
Testing recommendations and alternative diagnoses.
Lists of doctors by State or Country and whether they are self pay or take insurance.
Summary of State or Country laws dealing with disability.
Resources by location for logistics such as transportation, meal delivery, household help and more.
A registry for people or organizations willing to advocate for the ill in their area.
Document packets including a personalized ‘quick resource guide’ for all medical personnel.
Symptom logs.
Treatments which have helped (some) and other recommendations.
Correction of the PACE information.
Summary of ME/CFS research theory including information about PEM.
Pacing guidelines.
Other helpful websites.
This list could go on and on, but one thing that strikes me is that helpful information is all over the place and Cort’s blog is one of the few sites to find so much all in one place–but sometimes it is necessary to do a lot of looking, even in one site.
I know what I am asking is something I cannot entirely do myself because of my own fatigue, but if someone set up a clearing house site (at least a broad outline and category list), easy to use, then many people could contribute to it–kind of like Wikipedia. (And here I have to apologize for not getting my own EDS contribution done–yet. I’m having some energy problems of my own. ;-( ).
Cort, might you set up a link so any of us could start working on the outline (table of contents)? I’m not all that computer savvy, but if it was easy enough to drop information somewhere, maybe someone could edit and paste it into appropriate places.
Well, that’s my pie in the sky idea… I’m tired now…
Again, Amber, brilliant!
I really appreciate this blog and the thoughtful comments.
I want to add that we also need safe housing, communities where we can live safely together and we need to address homelessness.
We need to not be forced into poverty, isolation, homelessness and death because of all the things that are working against us at every turn, including advocacy that isn’t advocating from this perspective.
In 2019, Kenneth J. Friedman wrote https://www.frontiersin.org/articles/10.3389/fped.2019.00131/full
“Despite HIV/AIDS currently being considered a manageable disease, the proposed U.S. HIV/AIDS budget for 2018 was $32 billion of which 85 % ($20.7 billion) was for domestic care and treatment programs, 9% ($3.1 billion) for domestic care and housing assistance, 7 % ($2.2 billion) for domestic research, and 2 % ($0.7 billion) for domestic prevention (52). There are no domestic care, treatment, prevention, or housing programs for ME/CFS patients. For ME/CFS, a disease estimated to have more than double the number of patients, and with a quality of life judged to be as or more diminished than that of HIV/AIDS, the disparity in patient care and patient benefits is unsettling.”
There also seems to be too many conflicts of interest in our community. We are expected to tell our stories but what we really need is for our organizations and advocates to be telling the history of what has happened to us on a TIMELINE and NAMING NAMES!
We need to be using this history like we use the IOM report. The media needs to be covering this. ME/CFS is a huge social justice issue DECADES LONG! (I have personally been sick since 1983 and have been bedridden since 2007.) Without doing this, I feel like our history is being whitewashed further by our own community while we are disappearing and dying.
There is a lot of information here https://illustratorinterrupted.blogspot.com/2021/05/i-caught-virus-and-never-recovered-part.html?m=1 and other places that needs to be compiled and put together in easily usable and authoritative ways. I would love to land on the homepages of our organizations and clinician coalition and have it show the social injustice history before even getting into the medical and research information!
Also, I think that our disease is not being described accurately in ways other people can understand because it is not being described COMPREHENSIVELY, explaining how all the symptoms INTERACT TOGETHER in our SYSTEMIC DISEASE. Naming a few symptoms doesn’t describe the COMPLEXITY of the DISEASE. I think this is a huge hurdle we never get over.
I hope this all makes sense. I’m too sick to write more.
Lastly, if people can, please get involved with this #DemolishDisabledPoverty.
I forgot the link.
#DemolishDisabledPoverty
https://twitter.com/hashtag/DemolishDisabledPoverty?src=hashtag_click
A fantastic article about absolutely horrible experiences.
What is happening with the nanoneedle upgrade? The existence of a definitive diagnostic test to prove dysfunction, as published in PNAS, would have to be a pretty good psychiatrist repellent, wouldn’t it? Who cares about specificity (to ME/CFS), surely sensitivity is enough to show it isn’t in anyone’s head? CBT/GET recommendations may still be another issue to contend with but keeping a home ground advantage and not ending up in a psych ward has to count for something.
I believe it is the year 2021 so why oh why is this excellent article having to be written? When will people start to be made more accountable?
I think you can prove ( objectify) ME with the help of:
1. EEG
2. measuring blood flow to the brain
3. Heart Rate Variability
4. dual exercise test
5. NK cell cytotoxic activity
6. autoimmunity
Is there any way of contacting Amber Ella directly? I’d like to speak with her about a matter related to this article and would rather not relay specifics here in the comments section. Thank you.
Susan, I was struck by the poignancy of your comments. I have neuropathy also, but not always. When I do, it starts around 2 or 3 in the afternoon and my face and head have a burning, tingling feeling. This generally goes away after dinner which makes me wonder if it is gut related.
I am able to function reasonably well, however, because of the treatment regimen I am on which boosts immunity. If you have not tried these, go to the https://hhv-6foundation.org/clinicians/immune-stimulants I have taken Immunopro for years; Nexavir and recently added fermented wheat germ extract. Nexavir which is a cream that you can get without a prescription is made from pig liver extract and is the latest reincarnation of Kutapressin. I am also using intranasal VIP for heart and gut complications. Immunopro and fermented wheat germ can be ordered from Amazon. Nexavir directly from the manufacturer and VIP, which does require a prescription, from a compounding pharmacy. Nothing works for everyone, but I hope something in this regimen may help you.
I remember I believe.. didn’t Cher have CFS/ME? I am pretty sure she got treated / over it. I don’t know how. if it worked and if anyone can find out maybe that is a way to get more people on a trial of whatever it was she had done ??
Brilliant brilliant brilliant
Hi so after reading all of these comments, is there a cure? or any special foods or vitamins to take?
Thank you Amber for you article. As a severe to very severe ME sufferer who has live in poverty for over 40 years, I have one addition to your statement:
“Very severe patients cannot manage their activities of daily living, doctors’ appointments, prescriptions, home health, nursing, and other services. They need a medical advocate who is somewhat knowledgeable about ME/CFS and can ensure patients meet their goals. ”
Some of us are still able to manage our own ADL’s and IADL’s, schedules of all home health care and social services. The problem is that the health care system is so privatized by industry that “management” of our care and lives is taken away from us especially if one is poor. Poor ME’s lives have been taken over by the tech, medical industry and by the social service system. Everything is data driven, and “coordinated” for us whether we are hurt by it or not. We need more agency not less. And if we get so ill that we can not speak or move at all then the system needs to allow is to choose our own appointed essential advocate, caregiver that we have entrusted to help us “manage” our care and lives. We need more people in the ME community who are able to, to fight for a health care system that is free and allows doctors and all practitioners to go back to being hands on and not having to constantly be proving their “value” into their computer in order to get paid. A system where all home health care is free, including all physician and all other medical home visits, ADL and IADL’s. There is bill currently in congress that could jump start this shift in our current dysfunctional system.
Factor V Leiden mutation is more common in Norway descent. I wonder if that parameter has been looked it in ME/CFS as well as Long Covid there. Would be willing to be there is an increased incidence in those patients with thrombophilic blood disorders. ??