


The BA.5 Omicron Subvariant: The Worst Coronavirus Yet?
Variants of Concern
The coronavirus has been evolving rapidly over the past 6 months. (Electron microscope picture from the NIAID. The protrusions are the spike proteins the virus uses to infect cells).
Many variants of the SARS-CoV-2 coronavirus have been found, but since the Delta variant showed up in Oct 2020, only six have been considered “variants of concern“. Today, only one lineage of variants of concern – the Omicron variants and subvariants – is being watched now.
Variants of concern increase transmissibility, produce a more severe disease, are better at evading the antibody response, are not knocked down as well by treatments or vaccines, or are harder to detect.
(Thankfully, no “variants of high consequence“, which produce increased rates of hospitalization/death, a significant reduction in vaccine effectiveness, and/or may be more difficult to detect, are circulating now.)
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!A Mutation Machine
Last year I read an op-ed that suggested that the coronavirus was probably close to exhausting its ability to mutate. Instead, with the emergence of the Omicron virus, it’s turned into a mutating machine. At the beginning of this year, BA.1 Omicron variant hit the U.S. and other countries hard – producing the most coronavirus infections ever.
By April, though, the BA.1 variant had been supplanted in the U.S. by the BA.2 variant and had become the dominant coronavirus variant around the world. The BA.2 variants’ stay at the top of the coronavirus food chain, was brief, however. By May – just one month later – the BA.2.12.1 subvariant had become dominant in the U.S. By July, the virus had taken another big mutational leap – the BA.4/5 variants were now dominant
At every step, the virus has become more and more transmissible: BA.2 was 30% more transmissible than the very contagious BA.1, and BA.2.12.1 and BA.4 and BA.5 are more transmissible yet.
As our attention has waned, as life has gotten pretty much back to normal and as mask wearing has plummeted, the coronavirus virus has been mutating like mad.
The Latest “Variant of Concern” is a Doozy
In The BA.5 Story, Eric Topol M.D. lays out what he calls “the worst version of the virus that we’ve seen”. Topol is the real deal. A cardiologist, scientist, and author, Topol is the founder and director of the Scripps Research Translational Institute, and a professor of Molecular Medicine at The Scripps Research Institute. He’s published over 1,200 peer-reviewed articles, led clinical trials in dozens of countries, and is one of the top 10 most cited researchers in medicine. In 2016, he received a $207 million NIH grant to co-lead the Precision Medicine Initiative
He’s quite worried about BA.5 and what will inevitably follow it.
A New Virus Altogether?
The BA.5 variant first appeared in South Africa where it took one month for cases to rise from 1,000/day to 10,000/day. Hospitalizations and deaths did increase but not to previous levels. Next, BA.5 moved onto Portugal where, despite high vaccination rates, hospitalizations neared their previous Omicron peak. The New York Times noted that wherever the BA.5 variant has been able to settle in for a while, it’s produced a significant increase in hospitalizations.

With regards to community transmission – the CDC on July 6th reported that the U.S. is back in the red again.
Since then, it’s been moving fast. A month ago, BA.5 accounted for only 10% of cases in the U.S. Now it’s the dominant variant in the U.S., Canada, the U.K., and Europe. The 15% U.S. positivity rate – which tracks the percentage of positive test results – indicates the variant is spreading fast. The CDC estimates that the level of community transmission is high in more than 87 percent of U.S. counties and remains substantial or higher in 93% percent of counties. Basically, the U.S. is back to being almost all red. Across the world, cases have spiked 30% in two weeks We should know the impact it will have in the U.S. over the next month or so.
The earlier Omicron variants were more contagious but less severe because they were more likely to infect the upper respiratory tract (nose, sinuses, larynx) than the lungs. ( Anyone believing that the earlier variants were benign should read what happened to Aaron Teasdale – an adventure traveler and writer.) A recent report, however, found that the BA.4/.5 subvariants have evolved to target the lungs again – possibly making them more dangerous.
Immune Escape Artist
The BA.5 subvariant takes, as Topol puts it, “immune escape, already extensive, to the next level.” BA.5 is also far more transmissible than subvariants that came before it (BA.1, BA.1.1, BA.2, BA.2.12.1, BA.4).
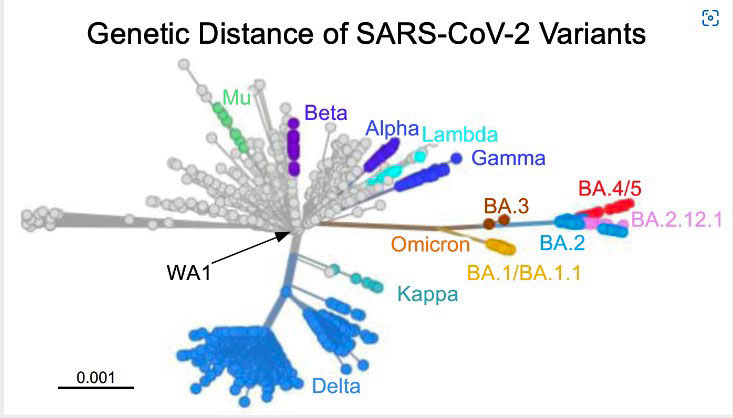
Topol shows in a series of diagrams just how different BA.5 is. Genetically, the Omicron created a branch of its own. Then the BA.4 and BA.5 subvariants created new branches off that branch. Their spike proteins – the part of the virus used to get into our cells – are simply off the charts different from even the past BA variants. Some of those genetic mutations extend to other parts of the virus as well.
Multiple studies have shown that the BA.4/BA.5 variants produce the lowest levels of neutralizing antibodies in humans yet. Introducing the BA.5 variant to a hamster produced the most severe disease yet.
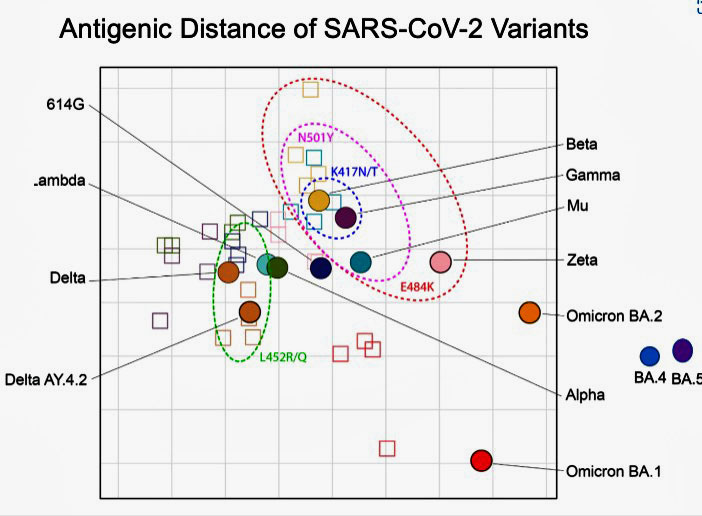
With regards the antigenic distance or the differences that have evolved in the genetic makeup of the spike protein that the virus uses to infect the cells – BA.4/5 are off the charts different.
With regard to its “fitness” – a term used to assess how fast the virus is reproducing, and how well it’s able to evade the immune system – BA.5 is basically off the charts more fit as well.

A recent report from the Kirby Institute in Australia indicates that BA.5 is more like the Delta variant as regards infectivity (i.e. it’s more able to infect cells.) as well. With regards to “fitness” or the ability of the virus to reproduce and evade the immune system – the early BA variants that produced the most death and disease yet – were monumentally more fit than the earlier variants. BA.4/5 – not seen in this chart are even more fit.
BA.5 is so genetically different from previous iterations of the SARS-CoV-2 virus that one researcher has called for it be given its own name – SARS-CoV-3.
Hospitalizations and Deaths Still Low in the U.S.
The good news, of course, is that hospitalizations and deaths are still far below the January peak of this year, and it doesn’t seem that anyone expects that kind of peak again. The subvariant is so different, though, that it’s hard to know exactly what will happen.
Given that vaccine effectiveness against hospitalization and death dropped from 95% for the Delta variant to 80% for the initial Omicron variant, it’s reasonable to assume that’s it going to drop more with BA.4/BA.5. People who are unvaccinated still make up a lion’s share of deaths, but the percentage of vaccinated people – particularly in the elderly – who are dying has increased.
The boosters still seem to be helping, however. The California Department of Public Health recently reported that unvaccinated individuals were more than five times more likely to get COVID-19, 7.5 times more likely to be hospitalized, and 14.5 times more likely to die from the coronavirus than people who had been vaccinated and boosted. Over the past nine months, approximately 234,000 people in the U.S. alone died who would have survived if they’d been vaccinated.

Hospitalizations and deaths among the vaccinated have started rising, but note that almost all of them occur in the elderly. Vaccination still provides substantial protection.
More data is needed, but one study suggested, interestingly enough, that vaccination does not seem to protect against long COVID. We’ll know more about the effects of BA.5 on hospitalizations and deaths over the next couple of months.
The Coronavirus Booster Poll
If you’ve had one or more coronavirus boosters, please tell us how it went.
Coronavirus Booster Side Effects Poll (3)
Reinfections Make Things Worse
A recent sobering preprint study found that instead of getting better at fighting off the virus, the body seems to get worse at it. The more times a person gets reinfected with the virus – the worse off they tend to be. Given how well the virus is adapting to evade the immune response, this outcome may not be surprising, but it is different. Reinfections were considered rare until the Omicron variant hit.
Most people who were infected with Omicron were infected with the BA.1 variant, but the BA strain has mutated so rapidly that these people have only “limited cross-immunity” to the BA.2, BA.2.12.1, BA.4, and BA.5 variants.
A large study that looked at hundreds of thousands of people found that death rates, cardiovascular complications, and adverse lung outcomes – doubled in people who were infected more than once, and the risk of being hospitalized tripled.
The rates of people experiencing fatigue, musculoskeletal, and gut problems jumped up dramatically. While the worst hit occurred early in the reinfection, some risks remained elevated six months later. Interestingly the three symptoms most associated with ME/CFS and long COVID – fatigue, gut, and musculoskeletal symptoms – were not significantly elevated after six months – suggesting that the risk of coming down with long COVID may not be elevated by a reinfection.
Long COVID
There is some good news about long COVID. A symptom app tracking study found that the early Omicron variants may produce about less 50-70% less Long COVID than the Delta variant did. BA.5, though, may be producing a more serious illness and producing more infections in the lungs. Time will tell.
Uncertain Future
Falling Behind – the Fall Vaccines
The new vaccines expected in the fall that were developed to address Omicron were directed against the BA.1 variant – which is long gone. A recent Nature paper that dug deep into the immune response against the Omicron variants concluded that Omicron variants are “continuously evolving under immune pressure” and pose “great challenge(s)” to the idea that a prior infection and/or vaccination will be able to produce herd immunity. The authors worried that the next crop of vaccines may not be able to “achieve broad-spectrum protection” against the new variants.
At the beginning of July, the FDA told vaccine manufacturers that they needed to produce a vaccine targeting the BA.4/BA.5 variants by fall. That puts the vaccine makers and the FDA in something of a time crunch. By the time Pfizer’s and Moderna’s BA.1 targeted boosters were approved, BA.1 had been supplanted by very different versions of the virus.
In order the get the new vaccines out by fall, the drug makers will have to start manufacturing the boosters en masse before they’ve been FDA-approved. Pfizer has said it can tweak its mRNA-based vaccine pretty quickly.
One report, though, stated that people who have been vaccinated or have been infected still carry enough of the neutralizing antibodies that protect them against severe disease and death. It’s the levels of the “lower neutralizing antibody levels” that fend off the virus that have dropped – thus we have more infections but not as much hospitalization or death.
New (Old) Vaccine in Town
A new vaccine – the Novavax vaccine – is coming to the U.S. Recently FDA-approved, the Novavax vaccine is a more traditional vaccine that directly injects the spike protein – plus an adjuvant that enhances the immune responses to the protein – into the blood. If you’ve had the Shingrix vaccine, it’s similar to that.
Manufacturing problems left the vaccine two years behind its predecessors. While it was very effective against earlier strains of the virus, it’s not clear how effective this long-delayed vaccine will be against the Omicron variants. (Novovax says its data shows that it will provide substantial protection and that a BA.5-oriented version of the vaccine should be available by fall.) As with the mRNA vaccines, very rare cases of myocarditis in young people were found.
With the U.S. dumping tens of millions of unused vaccines, it’s not clear that there’s much demand for Novavax, but it does provide a more traditional alternative to the mRNA (Pfizer, Moderna) and adenovirus (Johnson & Johnson) vaccines.

Eric Topol decried the “COVID Capitulation” he believes has occurred.
COVID Capitulation?
Eric Topol, in a May blog titled “The COVID Capitulation” – which was published prior to the emergence of BA4/5 – decried the lack of attention given to the add-on effects of the continuing spread of the coronavirus. He estimated that the real number of cases was probably at least 500,000 per day – far greater than any of the U.S. prior waves except Omicron.
Cases of long COVID, and substantial amounts of sickness, hospitalizations, and deaths were resulting, yet the pandemic was being treated as if it was largely over. With the U.S. seeing over 175,000 COVID deaths in 2022 already – 10x that expected from the seasonal flu – and with much better vaccines than for the seasonal flu available – Topol calls the high death levels “unacceptable”.
Forget Variant Chasing – Instead, Create the Coronavirus Vaccine to End all Coronavirus Vaccines
How long the vaccines can be expected to hold such a rapidly mutating and spreading virus at bay is unclear. The virus has changed so much and so quickly that a prior infection – even one as recent as a month ago – may not provide much benefit for those infected with BA.5.
Two critics of the fall BA4.4/BA. 5-based vaccines argue that they will probably provide minimal improvements, and that instead of spending increasingly scarce funds (given Congress’s unwillingness to devote more funding to COVID-19) on a massive nationwide rollout, funding should go to producing next-generation variant-proof or nasal vaccines.
The Gist
- Variants of concern are coronavirus variants that: may be able to increase transmissibility, produce a more severe disease, are better at evading the antibody response, are not knocked down as well by treatments or vaccines, or are harder to detect.
- Only one coronavirus lineage – the Omicron lineage of variants – is producing “variants of concern” right now. The Omicron variants hit the U.S. hard at the beginning of this year, producing high rates of infection, hospitalization, and death.
- Since then, though, the Omicron variants have continued to evolve with stunning speed, with each variant becoming more transmissible and “immune evasive” than the former. The new more contagious variants produced more infections but proportionately fewer deaths, possibly because they tended to infected cells in the upper respiratory tract but not the lungs.
- The latest subvariants – called BA.4/5 – resulted in an evolutionary leap for the virus. BA.5 is so different from the earlier variants that one researcher called for it to be classified as a new coronavirus.
- The BA.5 variant’s “fitness” (its ability to reproduce and evade the immune system) has been called “off the charts” stronger than the past variants. This variant is so different that some researchers worry that even a recent infection from an earlier Omicron variant may not provide much protective immunity.
- BA.5 first showed up in South Africa where it rapidly increased infections as well as hospitalization and deaths – but not to the extent that had been seen with some of the earlier waves. The variant then moved to Portugal where, despite high rates of vaccinations, it produced large numbers of hospitalizations.
- It took just a month or so for the BA.4/5 variants to become – just recently – the dominant coronavirus strain in the U.S. One worry is that some early (but preliminary) data suggests these variants may be infecting cells in the lungs. We will see over the next month or so the impact it will have.
- The vaccines were designed to protect against a different variant altogether and their effectiveness against hospitalization and death has waned by about 20%. (The waning, however, is concentrated in the elderly. In other age groups they remain highly effective.) Studies suggest that over 200,000 deaths in the U.S. could have been prevented by vaccination over the past 9 months.
- Some evidence suggests that the vaccines and/or past infections continue to produce neutralizing antibodies that protect against the most severe consequences of the virus. Antibodies that quickly tamp down the virus, on the other hand, appear to be waning.
- In contrast to past coronavirus waves, reinfection has become common. Studies indicate that people who are infected with the virus more than once experience greater rates of hospitalizations, cardiovascular complications, etc.
- Interestingly, rates of the symptoms associated with ME/CFS/FM such as fatigue, gut, and musculoskeletal symptoms, do not seem to be increased long-term in reinfected people. Another study suggests that the early Omicron variants produce about 50% less long COVID than the Delta variant. It’s unclear, though, how much long COVID the BA.4/5 variants will produce.
- The FDA has instructed the drug companies to produce vaccines directed against the BA.4/5 variants, but whether they will be able to do so in the time span allotted is unclear. “Variant-chasing”, though, has become increasingly untenable given the rapid evolution of the virus. Efforts to produce a coronavirus vaccine that protects against all coronaviruses and their possible variations are underway.
- Treatment effectiveness is also starting to wane as the new variants evolve further and further away from the earlier strains.
- Nobody knows if the BA.4/5 variants will produce a little, moderate or large bump up in hospitalizations and/or deaths over the coming months, but the extreme contagiousness of these variants is producing recommendations to mask up in any crowded areas – inside or out. If you can handle boosters – they are recommended as well. If you’ve been boosted, please participate in the Coronavirus Booster Side-Effects poll on this blog and tell us how you did.
- Unfortunately, the coronavirus is expected to keep mutating and rolling out variants for the next couple of years. Thankfully, no “variants of special concern” which are both more contagious and more deadly have shown up. The virus, however, will likely continue to get better and better at evading the immune response.
Ten different research groups are reportedly trying to create the coronavirus vaccine to end all coronavirus vaccines, and three are in clinical trials. The Mosaic-8 vaccine, for instance, which uses 60 fragments from eight strains of coronaviruses to build the vaccine, has been shown to work well in animal trials. Phase I safety testing in humans is expected to begin next year. Meanwhile, results from a US Army-produced mega-vaccine phase II trial should be out soon.
Topol believes we should also be producing nasal vaccines that stop the chain of transmission in its tracks. (The coronavirus usually invades through the nasal passages.)
Those and better antiviral drugs are the key, Topol believes, but neither are receiving the priority, they should. The answer for Topol is an Operation Warp Speed-like initiative to produce variant proof as well as nasal vaccines – which should be able to stop transmission – to the fore.
Treatments Falling Behind as Well
As the virus mutates more and more, it’s also leaving some treatments in the dust. Topol is not big on the antiviral Paxlovid which he reported is “being increasingly recognized to have a liability of rebound with infectiousness in many people after the 5-day blister pack pill”. He also worries that we may see drug resistance – something that’s already been seen with remdesivir – crop up in the coming months. He noted that the rapidly evolving virus has “already blown through most of the monoclonal antibodies that were previously highly effective”.
Topol argues that “We urgently need more safe and effective medications, preferably pills, easily administered shots (subcutaneously, not intravenous or intramuscular), or inhalation treatments.”
Many promising treatments are in the pipeline, yet support for them has waned. It’s this lack of attention to the evolution of the virus, the lack of support for mask-wearing, for vaccinations, for the development of better vaccines, for better drugs that for Topol signifies “Covid capitulation.”
Uncertain Future
It’s clear that the Omicron variant has unleashed a swarm of unforeseen mutations. Topol believes that with millions of immunocompromised people providing the virus with a kind of feeding ground, the virus will continue to mutate and that we should prepare ourselves for the possibility of something worse than Omicron showing up over the next year.
Kristian Andersen, a viral evolution researcher at Scripps Research, agrees. Not knowing what the future variants will look like – but knowing they are coming – Andersen states “we can be certain that they’ll continue to be more and more capable of immune escape”.
While they haven’t produced more severe diseases yet, that could be just around the corner. With our immune protection against the virus waning, we could be back in the soup in the near future if the virus makes an evolutionary jump that increases its severity.
Topol ends by stating, “It’s frankly sickening to watch this virus continue to outrun us, knowing we are so damn capable of getting ahead of it.”
Action Plan
Topol says that there’s no doubt that a new coronavirus wave is coming. What we don’t know is how deep and long it will be. We do know that it’s getting harder and harder to evade this virus. Dr. Preeti Malani, an infectious disease physician from the University of Michigan, told Business Insider that “Those of us who’ve escaped for 2.5 years? It’s gonna be hard to escape this one”.
That’s been my experience. Over the past couple of months, four people in my immediate family – all of whom evaded the coronavirus for over two years – came down with it. They were probably infected with the early BA subvariants – and thus may now be susceptible to BA.5. All had been vaccinated and/or boosted and all emerged OK.
Here’s one ” BA.5 Action Plan” that has been proposed.
(1) Mask Up!
So much virus is around that the chances of being around someone who is shedding if you’re in a crowd are high – even if you’re outside. Dr. John Swartzberg from The University of California, Berkeley, recently told the San Francisco Chronicle: “The chances of being around someone outside or inside who is shedding virus is very high,” infectious disease expert.
Mask use is way, way down, but given the contagiousness of the BA.5 variant, its ability to evade the immune system, and the increase in hospitalizations it’s produced in a couple of countries, masking up again in public, avoiding crowded areas, etc. makes total sense – particularly for people with ME/CFS/FM.
(2) Consider Getting Boosted
Everyone can make their own decisions about boosters. I’ve been vaccinated and boosted twice and have done fine. Others have had real problems. If you’ve gotten through the vaccines or boosts OK, another booster now could help.
(3) Create a Get Paxlovid Quick Plan
If you’re high risk, have a plan for quickly getting access to Paxlovid. Paxlovid is apparently available for free across the US. The more quickly you take it, the better it works (also, you must start it within 5 days at the latest).
(4) Improve Indoor Air Quality
Maintain high levels of ventilation and air purity.
(5) Accept that We’re Going to be Dealing with COVID Variants for Several Years

Mutations found in the BA.2.75 variant of the virus which recently emerged.
The SARS-CoV-2 virus is expected to keep evolving for several more years and has recently produced an entirely different variant of concern called BA.2.75 (aka Centaurus). We don’t know much about BA.2.75, but its boatload of mutations may take immune evasion several steps beyond even BA.5. Calling the number of mutations in BA.2.75 “remarkable”, one researcher suggested that the variant could herald in the next wave of infections after the BA.5 wave, that is. BA.2.75 emerged in India but has been found in the U.S., Canada, Europe, Japan, etc.
One person, frustrated by the seemingly continual emergence of new, highly transmissible virus types, asked: “Why is the solution space so big for this goddamn virus?”. It’s a great question that no one has the answer to yet. One thing is clear, though – we’re not nearly done with the coronavirus.


Omicron is old news. Centaurus is the new variant. By the way: vaccinations against omicron don’t help anymore.
https://www.newstalkzb.co.nz/news/world/world-health-organisation-identifies-stealth-omicron-covid-strain-centaurus/
Good news for Pfizer: they can make a lot of money again 🙂
I mean the newest subvariant BA.2.75 you mentioned it brain fog 🙂
My husband has had covid for 1 week now. He just finished Paxlovid with no problems. Luckily, my adult son and I haven’t caught it yet from him, as we both have lupus. I’m vaccinated and had covid last December and my son refuses vaccination and hasn’t had covid yet. Hopefully, our at home social distancing works out for us.
Centaurus is the newest variant but its reach is limited so far. Time will tell about that. BA.5 is the variant that’s circulating across the US, Europe, etc. Both Centaurus BA2.75 and BA.5 are both Omicron variants.
As noted in the blog vaccines are still helping to protect against the variants. Their protection has waned in the elderly but they still seem to be protecting just about as well in other age groups.
The booster have a terrible efficacy….it’s obvious the vaccine is causing rapid mutations to survive.
We don’t know what were messing with.
These vaccines have injured a lot of people. I mean I know of three just in my circle. One paralysis…which stopped after a couple of months ( but who knows the complications long term), one a stroke, which they survived but that put him off getting any more and rightly so and one a young woman who developed cardiomyopathy.
Fair enough, if your worried, get it, but last year, we got very very close in the u.k. to talking about not allowing people who are non vaxxed access to other treatments.
The restrictions in the media and by big tech were verging on a form of totalitarianism.
It was only the waning of the vaccines effect, when people could see with their own eyes, that even tho they got vaxxed, they still caught the bug and at a similar severity to those who didn’t take the vaccine.
The vaccines never stopped transmission. That was a lie.
We need better treatment s than this vaccine . It’s just driving us round in circles.
I totally dispute any narrative that says it saved lives. I just don’t buy the research at all.
Like I say, it’s fine for people that wanna take it, but it’s never gonna stop covid. You’re just delaying the inevitable.
I’ve not been vaccinated and am still here, despite moderate debilitating CFS.
I’ve been regularly exposed to the virus. I got ill once. Never since.
There seems to be a pattern emerging, that those that get boosted keep getting sick.
I think this is a fair stance to have, this far into the pandemic. We need to recalibrate our treatments. The vaccines have a work rate of as little as four weeks…seems to be getting less each time
All I can report on is what the studies say Oliver and they say the boosters are still providing efficacy and that hundreds of thousands of people have died who would not otherwise if they had been vaccinated.
People with their own eyes, by the way, are no way to judge the effectiveness or not of vaccines. People get sick all the time with all sorts of things. The fact that something happened to someone around the time they got vaccinated means nothing unless a placebo-controlled study shows that people who got the placebo didn’t have that reaction. We do this big expensive studies to control for things like that.
I certainly agree that the vaccines have harmed some people with ME/CFS/F. This undoubtedly won’t convince you but the fact that the studies are picking up evidence of very, very rare cases of heart inflammation and that is being reported upon and people are being warned about that – says something. Fatigue and side effects like that I’m not so sure.
Ha..imastounded anyone still buys into what is obviously a massive heist.
The vaccines just don’t work. How it was sold to us was hogwash. It blows my mind that anyone with m. E. Believes a word that comes from these pharmaceuticals.
I used to be very pro doctors, and science and orthodoxy, but profit and medicine, plainly do not mix.
When will everyone wake up.
Dude, you’re coming here spraying your (unverified) personal anecdotes around and pretending like they outweigh published scientific research. This is no help to anyone.
Oliver I 100% agree with everything you said!!! When will people wake up? I got MECFS BECAUSE OF VACCINES, which YES that’s confirmed by my MECFS specialist, also I’ve talked to THOUSANDS who also got it from vaccines! When will people start listening to the experts (scientists, doctors etc) that are being blocked and deleted from all social media and main stream media and look at what they have to say? That’s who I follow and trust 100%! Also people can go to VAERS website and see for themselves all the vaccine INJURIES AND DEATH from the covid vaccines!!! Then if you research the fact that only 1% is actually reported to VAERS based on several studies including Stanford etc then multiply that vaccine injury and death number you will clearly see that more people have been injured and killed by the covid vaccines and “treatment” than died from actual covid which has a 99.97% survival rate.
These variants are being CAUSED BY THE VACCINATED!!! It even says in the vaccine trials that THE VACCINATED are the ones shedding this crap!!! Hell the man who came up with mRNA vaccines said he would NEVER take one (Dr Robert Malone). If anyone wants some real true information and FACTS then there are plenty of sources out there that can give it to you but the government and main stream media definitely aren’t trustworthy!!! Also there were patents on covid DECADES ago!!! It’s a bioweapon and everyone that’s taking the vax is taking the bioweapon! Very very sad that people just believe what they are told instead of looking at the facts on both ends of it and deciding for yourself who is telling the truth!!!
Actually, the consensus is more that the variants are being caused by the virus circulating for long periods in people with compromised immune systems. When treatments don’t knock out the virus they can apparently cause the virus to mutate. Here’s what happened with one person who eventually died from the virus. It’s really rather fascinating if a bit horrifying.
https://www.scientificamerican.com/article/covid-variants-may-arise-in-people-with-compromised-immune-systems/
Robert Malone did not create the mRNA vaccines, either. He produced one paper 20 years ago and then basically disappeared from the field. They, like most advances, are the product of hundreds of researchers work. “The New York Times, in an article about Malone, reported: “While he was involved in some early research into the technology, his role in its creation was minimal at best, say half a dozen Covid experts and researchers, including three who worked closely with Dr. Malone.””.
https://en.wikipedia.org/wiki/Robert_W._Malone
He’s also regularly accused others of downplaying his work – it’s a theme that’s shown up throughout his career.
This is a complex subject. There is no doubt that some people did poorly with the vaccines. It’s also true that hundreds of thousands of lives were saved by them and hundreds of thousands more would have been saved by them if more people had been vaccinated. Everybody has to decide for themselves whether to be vaccinated or not.
Nobody should be swayed by anything assertions about VAERS, however. As has been noted many times if VAERS followed everyone who say ate a banana it would find people having heart attacks, strokes, etc. afterwards – not because the banana caused that but because these things are happening to people every day.
Large placebo-controlled studies that give the vaccine to half the participants and the placebo to the other half are the only studies that can determine the effects the vaccines have. It’s unfortunate that those studies have not been done in ME/CFS or FM.
Yeah, I trust “the Science” about as much as I trust anyone who tries to hard sell me on something they profit immensely from. And yes, the researchers get their grant money from Fauci who owns plenty of patents himself.
Have you seen those bizarre rubbery clots Embalmers are finding in many deceased? As in, not normal blood clots but never before seen beige colored clots which oftentimes are extremely long and oddly shaped?
Where’s the Media on this? Oh, how silly, Big Pharm is its sponsor. No story here.
That ClotShot makers openly have admitted they were wrong as they promised all would be well if you took their warp-speed product. Now they confess they cannot prevent infection nor spread, but certainly can lead to heart inflammation & attack, stroke, seizures, along with many other horrific complications such as miscarriage and stillbirth. VAERS itself testifies to but a small portion of those who’ve learned this the hard way.
When will people wake up IS the question.
That’s why I love the Doctors at the FLCCC. They offer concrete ideas to help prevent infection and to treat it if it hits. They also offer protocols for those who sorrowfully must now live post “vaccine,”
but want to try to overcome their damage.
https://covid19criticalcare.com/
There’s actually been quite a bit of work on the strange blood clotting problems – in long COVID and recently in ME/CFS as well. These are separate from any vaccine associated clotting problems – I don’t know about those – but clotting seems to be an inherent problem in these diseases. A blog on that is coming up.
The NYT “reporting” on Robert Malone was a lie-filled hit piece over which he has threatened to sue.
Many major media outlets took $1B in Gov’t money to portray vaccines in an only positive light, reducing them, on this topic, to just basic gov’t propaganda.
This from a simple Freedom of Information Act request:
https://www.theblaze.com/news/review-the-federal-government-paid-media-companies-to-advertise-for-the-vaccines
Dr. Malone prolifically posts on Substack; people can read for themselves and decide if his info (much of it Science–that thing we’re told to trust) is useful… https://rwmalonemd.substack.com/p/update-regarding-omicron-ba5
Thanks for this blog, Cort.
In NYC, it’s extremely difficult to protect oneself given the flood of tourists we have coming in and refusing to wear masks. Despite having three shots (my doctor advised me to wait to get another in mid April) I came down with Covid at the end of April. Despite paxlovid, it’s been a difficult experience. (No one mentions it, but paxlovid is a tough drug, too – terrible side effects and bad interractions with a host of other medications).
At this point, I don’t want to leave my immediate neighborhood but the tourists flood in here too, and seem to think that they don’t have to wear a mask because they’re not at home. Go figure.
I wish our public officials — especially our current ones in NYC — could get the word out better. Thanks for your contribution.
My sister and her husband went on Paxlovid and yes, it sounded like a rough drug indeed. I’m in Phoenix right now and mask wearing is down to an all-time low – maybe 10-20 percent.
Cort you can’t have it both ways. I remember telling you last year that even if everyone got vaxxed there would be immune escape.
I repeat, we don’t know what we’re creating. I said this last year. We can drive a variant that wouldn’t occur naturally because of the pressure.
Regarding judging with your own eyes.
We both know how these big corps operate. The fact your asking for vaccine reactions shows how up in the air and by the seat of your pants this is.
I’m suprised anyone with m.e. believes the rubbish when they’re shown to manipulate and hijack information.
Zero covid policy didn’t work in China. And that’s as brutal as you can get.
The vaccines have a supposed efficacy of 4 weeks coverage…I mean , come on!!!
Paxloid et Al are just desperate money grabs.
I just can’t see how anyone still believes this is controllable and that the vaccines are safe.
Like I say, you can’t have it both ways…the vaccines didn’t cause any of these injuries I speak of, just coincidence and yet the fact that many 90 year olds died with covid up their nose was the cause of death when they had severe medical illnesses that had them hanging in the balance. What other viruses did they have in their nose.
The risk reward is the thing. Finally in the u.k. they’re seeing sense.
Over 50s and vulnerable s are getting an autumn Vax…if they want it.
Great, that’s how it should’ve always been.
There’s plenty of epidemiologists who don’t agree with mass vaccinations, who don’t agree with their studies…I’m pushing back on this because, here in the UK our hysterical response has put into action a terrible tsunami of collateral damage. Cancer ) heart diagnoses missed etc. Violence up, many excess deaths. Children’s mental health has been affected, yet the average age in the UK if someone dying with covid was 82..the average lifespan is 81!!!
People go on about long covid.well first there’s no real evidence that vaccines cut it out as they can also induce long covid .
Also, nearly everyone will get this virus. It’s a coronavirus. Fine if you feel it protects you, take it, but ramping up hysteria is the last thing we need. So much damage and death has been caused by our response, that will last decades.
Sweden was planned for its covid response, but it saved a lot if lives that way.
There is an exhilarating fear around what is essentially a cold for most people. A very nasty cold. My sister just had it again and thought it was hayfever.
I’m saying we need perspective.
I’m in the same boat as you. I have m.e. but I’d rather let my body fight the infection that out smthg into my body that has no ling term safety data. Crazy to me
It’s a mistake in logic Oliver to say that because the vaccines didn’t prevent immune escape that they’re not effective. Since the vaccines rely on boosting the immune response they’re not going to be so helpful in an immunocompromised person who can’t mount a strong immune response anyway.
The vaccines do seem to help with transmission but that’s not their intended purpose – their purpose is to reduce hospitalization and death and and according to the studies they’re doing that in spades.
Yes, COVID-19 is mild in most people and yes we would do things differently if we did it all over again but please don’t blame people for getting a once in a century pandemic event wrong. We were all making it up as we go. If it happens again we will do better.
That “nasty cold” has killed over a million people in the US. In 2021, covid was the leading cause of death for people ages 45 to 54. (https://www.msn.com/en-us/health/medical/covid-killed-30000-middle-age-people-in-2021/ar-AAZndDI). That’s not what nasty colds do.
Can’t fill out the survey. It only is allowing one choice per question rather than “all that apply.” Am I the only one? I’m on MacBook.
Same here
Yes, same here, can’t pick multiple options
Sorry to hear that. The initial poll had a mistake with the symptom question but it was fixed or I thought it was fixed. Some people have been able to check several symptoms. We may have to disregard the answers to that question, though.
No Cort…my point is, the last few years you’ve been selling this. Fine it’s your view, but as this is a reaction forum, I’m entitled to call out your mistakes in logic.
At the time, you were angry at what you saw as political affiliation affecting people’s to decision to take the Vax.
Whilst that was one layer of the refuseniks, there were also just many concerned individuals, like myself who had reason to believe a trial so hastily put together, and with a new technology( yes 30 years development blah blah, still a new technology) was good reason to not throw caution to the wind. . Boris Johnson warned us that we would all know someone who has died of this , I still don’t. I know people have died. I know it’s a serious illness for some and it killed a lot of very old people and some younger people and caused a lot of pain. But, and now as I saw in the observer today ( the left wing are finally starting to acknowledge they put themselves first in this) kids have been really badly affected mentally and developmentally. For a disease that had nothing to do with them. What are they vaxxing kids for???
I remember at the time, your false logic. You bemoaned the fact that there wasn’t enough uptake of the Vax, and if we only pushed forward and stepped up this would be all over.
I said at the time, not like I’m a genius, just realistic, that this is s coronavirus, vaccines won’t beat it and everyone will get it,. Vaccinating everyone would make no difference except to perhaps the ones who need it. So get it! But don’t make the rest of us!!!
The vaccines don’t stop transmission or illness!!!! Just severity..apparently…but if you remember we were fed a string of falsehoods.
Don’t worry we can change the Vax to adapt to variants every six weeks ( at the time I pointed out, just logistically getting this into arms would be impossible, but out of fear, the leftists in these arguments said I was trumpian. I’m on the left myself but could also handle reality.
They said transmission would be stopped, no, then disease, no, then we’ll it stops death. Does it? Or have just the most vulnerable been killed?
The way big tech has strangled any debate, that is a big clue that there was an agenda. I don’t know what. Probably just money.
But I guarantee, whatever they put in this new Vax, we will have this same conversation in two years time.
I assert, we do not know what we’re doing here in many different ways and we need to take stock and not carry on with these lockdowns that harm the majority to “protect” the vulnerable. And have some independent studies into vaccine injury.
I asked my doctor who has around 100 fibro/ m.e. people on her books..there were a lot of injuries and worsening of symptoms. A fair number of worse for a while then better and a couple of improvement s. The majority were made worse tho and for me , along with all the rest of the evidence of injury, I feel I made a wise decision.
With or without the Vax, we will all get covid. If you feel the Vax protects you, that is great and completely within your rights.
I’m really wary of the coercion that’s gonna come upon us again to take this technology inside our bodies. The Amish have done just fine.
I know a lot of vulnerable people say it’s unfair for everyone else to be able to get on with their lives whilst they stay indoors. Well most vulnerable people stay indoors anyway!!! Why force healthy people to live the sane life?
Fine adopt standard pre pandemic WHO protocols and take our time in doing some non rushed careful research into this
I guess it depends on whether you trust the science. I read a book on the development of the mRNA technology. It was developed by very well thought of and careful researchers. Because these trials were so momentous and of such import – and were overseen by top people in the field – I trust them. Actually, this topic was of such significance and therefore had so many eyes on it from so many different people and institutions that I trust it more than just about anything else. It’s really a fundamental matter of trust and I chose to trust.
Of course we’re flying by the seat of our pants. I think we felt that we had to do things quickly – that the virus was spreading fast – that the economy was taking a big hit – and we had to get those vaccines out. The mRNA vaccines were able to be developed the quickest and they happened to be brand new. Frankly, I was surprised that the drugs companies were willing to take such a change on such new technology. I actually came to the conclusion that the technology must be effective because they were willing to take such a chance on it. After all – if it blew up in their face – they were going to be in real trouble.
We’re going to make mistakes and we have. I don’t think anyone would want to do a total lockdown again. I think the consensus is that that was probably too much. Hopefully, we’ll be better prepared next time.
Oliver: You take a very reasonable approach to the issue. I, too, refuse to take an experimental so-called “vaccine.” I’m acutely aware of the VAERS data, people I know who’ve been seriously injured by the jab and the deliberate repression of open debate on the entire matter, as well as the tremendous positive outcomes from Ivermectin and other repurposed drugs and naturopathic approaches to viral prevention and treatment. But so few are aware of these things because of the coordinated attack by various Governments and the Big Pharma indebted Media against alternate options to their tightly controlled narrative. They have innocent human blood on their hands.
Not only have I suffered from CFS-ME severely at two separate points in my life, I also have a blood clotting disorder and almost died from a DVT while much younger. My Pain Doctor begged me to get the jab, telling me it was my “winning lottery ticket.” I explained to him several times the last thing I’d do is intentionally permit spike proteins to swim in my already seriously compromised vascular system. I’m unapologetically proLife, and that includes for my own life as well.
I do, however, wear an N95 mask with a K95 mask over it every time I go into enclosed spaces such as grocery stores, doctors’ offices or to church. I also wear a large plastic goggle over my glasses. It’s all incredibly annoying and uncomfortable, but I do what I have to do. Plus I never stay out anywhere for over an hour, so that helps as well.
I also take Ivermectin prophylactically. I take Zinc, Quercetin, Vit D, Vit C, Lumbrokinase, etc. When I come home from my occasional outings I immediately put my clothes downstairs near my washer, shower, gargle with Crest mouthwash, rinse my nasal passages with previously boiled water with saline and a few drops of povidone iodine, as I learned a long while back about these life saving strategies from the wonderful doctors at the FLCCC. I watch their Wednesday night Zoom meetings and stay current on their updates. They’re always learning and adjusting their approach to the bizarre reality we’re facing.
So far, so good. But I have a plan should the worst happen, as well. Having lived through the indescribable nightmare of CFS-ME and before that almost dying from blood clots at 21, I have no desire to give up or to give in to the wicked liars who’ve threatened, bullied and deceived far too many.
God bless us as we keep on keeping on.
If there’s any good news, it’s that researchers of a nasal vaccine couldn’t include an ‘adjuvant’ (because it caused Bell’s palsy) So instead they made the nasal vaccine without any adjuvant and it amazingly still worked just as effectively at producing antibodies on the mucus membranes of the nose and throat (which is the crucial entry point for the coronavirus). Many times more antibodies develop on the mucus membranes with a nasal vaccine compared to the current vaccines. Which means people won’t be spreading Covid either.
I believe that adjuvants in current vaccines are half the problem for people with ME/CFS who react badly to vaccination. The reason is an adjuvant is designed to wake up the immune system to create a robust immune response while the viral antigen (virus parts or shapes of viral protein) is present.
Unfortunately in some people with ME/CFS that response becomes too aggressive ( https://file.scirp.org/Html/17-2100362_24744.htm ) as seems to set off a runaway reaction that lasts months, if not permanently worsening the patient (as has happened to me with a flu vaccination 6 years ago. I went from mild to severe ME/CFS)
Some ME/CFS clinicians describe adjuvants as “turbocharging” an immune system that’s already dysfunctional.
So that’s possibly partly why some of us end up worsening after vaccination.
A few studies have since shown that the current mRNA vaccines lipid nanoparticles are highly inflammatory and are probably what’s providing the adjuvant type effect. ( https://www.biorxiv.org/content/10.1101/2021.03.04.430128v1 )
So hearing that researchers have removed the adjuvant from the new nasal vaccine and only having a viral protein or viral particles sprayed onto the mucus membranes, could be the answer we more vaccine vulnerable ME/CFS folks are looking for.
A nasal vaccine spray would be almost as if we had caught the first stage of Covid naturally, except these virus parts aren’t able to infect deeper via replication. (And won’t be sitting inside our lymph nodes or circulating in the blood 8 weeks later as was discovered recently with a mRNA vaccine. Published in CELL https://www.cell.com/cell/pdf/S0092-8674(22)00076-9.pdf we all know lymph nodes function in ME/CFS are already problematic. Perhaps some of us aren’t able to rid mNRA and the spike protein out of the lymph nodes as well as healthy people? Hence the prolonged sickness after mRNA vaccination)
So because the nasal vaccine isn’t injected, it shouldn’t cause a systemic body wide inflammatory response, (especially if it’s instead actually the spike protein itself that maybe also causing the inflammatory response with current injectable vaccines). Instead the nasal vaccine antigens are localised to the mucus membranes for a separate immune response.
Even better the antibodies produced on the mucus membranes last much longer, so have the ability to fight off recurrent infection many months later.
This article explains it well… (including an inhaled vaccine for if the virus starts infecting via the lungs again)
‘Why Nasal Covid Vaccines May Make Better’ Boosters – The New York Times
https://www.nytimes.com/2022/02/02/health/covid-vaccine-nasal.html
Hopefully people with ME/CFS will do a lot better with nasal vaccines. Although we can’t be certain they do seem promising.
Brendan, thanks for the info about the nasal vaccine and their lack of adjuvants. Definitely a vaccine I would consider getting.
Use of adjuvants in vaccines would logically trigger ME/CFS immune systems into overdrive, which is what I experienced with the second Pfizer dose 14 months ago. My spike protein antibodies, according to the Serimmune study I joined six weeks ago, are still elevated. No surprise there, since my CMV, EBV, and HHV-6 antibodies have never been anywhere near the normal range, even after 20 years. And I haven’t been exposed to the actual coronavirus, given the near-total absence of antibodies to the proteins not found in the vaccine.
Adjuvants are a nasty piece of trickery for immune systems like ours. It’s why several doctors have told me to avoid the Shingrix vaccine at all costs, even though I had chicken pox as a kid. I’ve had Guillain-Barre Syndrome in the past which took a year to resolve; it’s neuropathy and muscle weakness all over your body. And the adjuvants in the Shingrix vaccine increase the risk for even healthy patients developing GBS. I’d rather deal with shingles than go through Guillain-Barre again!
I’m hopeful the nasal vaccine will be available in the near future before BA.5 runs rampant.
(Rick’s comment was removed. I recognize this is a heated topic but this is not a political blog – it’s an ME/CFS/FM and long COVID blog. Therefore this comment has been removed. Please try to refrain from discussing politics! Thanks – Cort)
I’ve seen plenty of political comments – including wacko conspiracy theories – on this site that are left to stand. I’ll take that as an indication that a nerve was struck by the truth of my remarks. In fact, knee-jerk reactions notwithstanding, there was nothing inaccurate in what I said at all. Wear N95 masks and social distance? That’s better advice than we are getting from virtually any quarter, as most who at least advocate for mask wearing are not making the crucial distinction between ordinary/surgical masks (which are rendered even more comically useless by the way most people wear them, with their nose and even mouth uncovered) and N95 properly fitted and worn.
Moreover, the very article by Topol that you reference in your blog post has a long section on U.S. political involvement, including editorializing remarks in regard to the “delusional” nature of Congress and specific mention of the current administration’s downplaying of the current situation and risk:
– – –
A Delusional Congress
With that handwriting on the wall, how could our government legislators turn their backs on funding critical initiatives to get us through the pandemic? This is frankly absurd, staring at millions of more Americans to get infected that is happening right now (no less the Biden administration has projected 100 million this fall/early winter) that will translate to an unknown number of more hospitalizations and deaths. Ironically, the same administration, via the CDC, is downplaying the risk of our current Covid wave as reviewed above….
– – –
So… If political commentary is the criterion for censorship, shouldn’t you edit (censor) your own article?
Actually, Rick I’m trying not to let this blog turn into a political food fight. That happened early in the pandemic – it was partly my fault – and I resolved not to let that happen again. I agree about the mask-wearing and Topol’s frustration with Congress is different as its not aimed at one administration; it’s aimed at “Congress”. Plus it wasn’t the focus of this blog. The blog was on the emerging variant – not how poorly one administration vs the other is doing at fighting it.
Fair enough on the food fight, Cort, but I think you’re being naive in regard to congress. I mean, one party or another is controlling the agenda there, right, and also being influenced by the admin – which he explicitly calls out. It’s clear that he’s pro-admin and is merely trying to constructively criticize, so maybe that’s the difference, as I don’t like to take sides and prefer to just call out reality as it happens. That’s part of finding solutions, in my opinion, as we really can’t afford to be blinded by political rhetoric and afraid to speak out when it comes to serious public health issues like COVID. That was the main point I was trying to make.
So just to clarify, I’m not saying any of this with any political agenda in the least. I only want the problem to be solved. And that’s not happening now, we’re actually going backward in many important respects, with NYT showing that cases are actually spiking to all-time highs, and (if you switch to 90-day view) are steadily increasing over the past few months: https://www.nytimes.com/interactive/2021/us/covid-cases.html
Why aren’t we hearing about this 24/7 like we did during the previous admin? Where is COVID on the nightly news? Have you watched any mainstream news lately? Rarely a word about it. Hmm. Why aren’t they discussing experts like Topol’s concerns? Don’t you think they would be (with their dramatic headline music and in their serious tones) if we were in the middle of the last campaign? You don’t think that emphasis (or lack thereof) is political in nature?
And all that plays to public perception and response to the pandemic, I believe. Because now, thanks I contend to the largely partisan political climate and resulting media coverage (or again, lack of coverage), we are seeing the majority of people act like the pandemic is over (as Topol also notes). Imo that’s a direct result of how media is approaching and distorting the issue – *for political reasons* – and it’s only making things worse.
So I think to ignore those realities is to ignore an important component of what actually is driving or at least directly influencing the course of the pandemic. We need a more accurate assessment of what’s happening, not less accurate – not less coverage b/c you aren’t actively trying to get one person out and another in – and calling out failures in our political leadership – which I have done, which Topol has done – is necessary, imo, as well as pointing to how these political realities are influencing public response to and the trajectory of the pandemic. And that’s true regardless of which side it is. So not partisan, only reality.
Honestly, I don’t think the lack of attention has anything to do with one administration or another. I think it’s more COVID fatigue – everybody wants to be done with it. I haven’t been paying attention. Some brought my attention to BA.5 and only then did I find what was happening. I was totally out of the loop.
No one really wants to hear about it anymore and the death rates while really still unacceptable – 300 + a day – are farm far lower than they were. The media has only recently started publishing about the new variants. The coronavirus doesn’t bring in readers like it did before and they are moving onto other things.
The same thing is happening with the Ukraine war. I used to regularly watch Youtube interviews with the generals on CNN, FOX, and others. That programming has almost totally disappeared. Only UK and Australia media outlets are regularly covering the Ukraine war now.
I don’t disagree that after two and a half years there’s a good degree of fatigue on the issue. And with supreme court decisions, mass shootings, and as you referenced a major war happening, naturally the news cycle will tend to shift to “fresher” topics that are momentarily capturing the public’s attention.
However, COVID coverage has virtually fallen off a cliff. It’s gone beyond fatigue and has entered the realm of denial. If the media and governmental authorities wanted this issue front and center, it would be. Clearly they don’t – they just want it to “go away’ (we all do, of course, but that’s not what I mean), and in my opinion those decisions are largely being driven by political agendas. Important elections are coming up in the fall, and the last thing this admin wants is their complete failure on COVID dominating the headlines and public consciousness.
We really need to face this issue squarely and demand accountability of our elected officials, in my opinion. This thing isn’t going away quietly, despite the attempt to sweep it under the rug. It’s only getting worse, and if the media wanted attention on it, believe me, they could manufacture that very quickly
and very easily, fatigue or not. They don’t want to, because it’s no longer an issue they can exploit to demonize the guy they don’t like, i.e. they can no longer politicize it in that way because now it’s
I’m not going to belabor this point, it’s just one part of the whole picture – though an important one imo. I can appreciate you wanting to keep the blog focused on the actual scientific aspects, and I think my frustration over the lack of progress just flared up on finding out more about this new variant – I hadn’t heard about it, either! That’s what I’m saying!! We’re not really being told, and it’s not all about fatigue, b/c if news had been reporting on this responsibly, I can say for sure that I would be interested. And I know I’m not alone in that. So ironically or not, I’m not really being political, but saying the politics on this thing have got to stop. Thanks for (mostly ;-)) letting me vent.
Cort I’m asking for accountability and not making the same mistake twice.
Us doubters WERE blamed and ridiculed for having genuine concerns.
We kept level heads. We told you the obvious consequences of this early on.
Most people on some level knew this was an overreaction. I don’t think many thought through the uncountable death toll that overreaction has set in motion. It will easily be more than any covid ” death toll”.
You’re making the same mistake again. Getting all riled up about a virus we can do very little about.
Never fly by the seat of your pants would be my advice…not when we’re dealing with children and anyone under 50 whose healthy.
Masks, fine. Social distancing fine, anything else is not gonna work.
Maybe in five years you will stop believing ” the studies”. It’s a corrupted system.
Come on!!! We know this!!! Were m.e. patients for god’s sake!
Anyway, I just don’t like the idea that we tried to warn you, the were not allowed to hold you accountable.
It’s not a once in a hundred year pandemic btw. There’s been a few fly’s with similar mortality levels and remember aids.
We gotta start being level headed and holding the powers that be accountable with I dependent journalism and the right to say what we want without being shared like we were. That’s why people like me are pushing back. We told you and were shamed for it…
Anyway..made my point.
I’m surprised to find you’ve picked up this one-sided story line, Cort. I’m not impressed. It takes very little research to find out that Eric Topol is sponsored by the Bill and Melinda Gates foundation and Apple. There are vested interests here! Don’t help them spread irrational fear.
I know the Bill and Melinda Gates Foundation has become “the devil” in some circles. I honestly don’t understand why that is. They’ve funded over $2 billion in anti-COVID projects – most of which is going to low-income countries to provide access to diagnostic tests, vaccines, and treatments https://www.gatesfoundation.org/ideas/articles/covid19-contributions. I’m all for those things.
I didn’t know there was any controversy about Apple. I see that Apple, Garmin, and Fit funded efforts to produce a mobile app to track COVID which Topol may have been a part of and as a cardiologist he’s promoted the use of wearables.
Any funding that Topol has received from any private foundation, however, is miniscule compared to the amount of grant funding he’s received from federal sources. He received for instance a $200 MILLION grant from the NIH to help lead the Precision medicine initiative. He’s published over 1200 papers in medical journals. He received a $35 million NIH grant to promote innovation in medicine. He’s one of the top 10 most cited researchers in medicine. He’s led clinical trials in over 40 countries involving over 200,000 patients and has edited over 30 books.
In short, he is the kind of guy that I trust.
So-called Big Tech and Big Pharma are the “devil”. Any good they do is dwarfed by the evil they commit. They won’t solve me/cfs or longcovid. They will find drug targets and provide technical aids that steal our personal information, so they can continue to make billions of the backs of sick people. They do not care about us.
And the drugs they give us will only make us ill in a different way in the long term. How many times do they have to screw us over, for people to wake up to reality?!
Given that the vast majority of people are not helped by supplements, diets, what have you – the answer is probably going to come from drugs or similar treatments. If you’ve priori decided to throw all those out the window – what do you have left? I don’t know if you have any answers at all? I urge you to keep the door open for drugs! Yes, they are powerful and can cause harm and people with ME/CFS have to be careful in particular but drugs are probably the answer. I was recently talking with my partner about the horrid rheumatoid arthritis her mother suffered from several decades ago. You don’t see many cases like hers anymore because the drugs are helping.
Health Rising focuses on scientific studies because they present the best chance to get at “reality”. That’s why All sorts of efforts are made – by matching patients with controls, by removing patients with confounding illnesses, with having the right numbers of participants in a study to provide statistical validity and then by assessing the statistics – that’s all in service of getting objective facts – of getting as close to reality as possible. It’s imperfect but it’s the best we have.
It’s true we never got people with ME/CFS into their own vaccine trials and that’s a shame because we are different. For the general population, though, I rely on the answers provided by very large (tens of thousands) vaccine trials in the general population. They are the closest to reality that I can find.
Mr Science and the CDC originally said the jab was to stop the contracting and spread of covid. That WAS the definition of vaccines. When breakthrough cases became the norm, the vax definition and purpose was changed to limit the spread and severity of the disease. Then they had to lower expectations even more, saying it lowered the number of hospitalizations and deaths. The stats also don’t count as fully vaxed, anyone who gets sick within two weeks of the jab, or who hasn’t had all the jabs recommended at that particular time. Most studies I’ve seen also go back to when the vax first became available, even though most of the people couldn’t have gotten it yet, so the number of sick unvaxed is bound to be much higher in comparison. Numbers can be manipulated to say just about anything you want them to say. Money, power, and ego speak pretty loudly about what they wants said. Not to mention that without double blind studies with separate groups for vaxed and deliberately exposed vs unvaxed and deliberately exposed, and then throw in the same classifications but all having already had covid, there is no accurate science on which to base the effectiveness of the vax. How can one prove a mild case was the vax and not simply the results of a less virile bug? I should also add that it’s a well known fact that historically, viruses tend to become less lethal overall as they become more contagious. The original covid was definitely a nasty bug, but unless it’s manipulated again in a lab, I fully expect covid to become more and more like the flu or a cold as time passes.
I don’t know that anyone said the vaccines would stop the transmission of the virus but if they did I encourage you to give them a break. I was really happy to hear that it stopped hospitalization and death! This virus came upon us unsuspecting and everyone was surprised that people were able to spread it BEFORE they had symptoms. That made it very difficult to stop. It took a long time to recognize that it was airborne. First we were most concerned it was spread on surfaces. We’ve learned a lot about this virus – it just took time.
Again, it depends if you choose to trust the science. As I stated I choose to trust it. You obviously feel it was manipulated. I don’t. Therein lies the difference!
Tell that to the farmers in India
Whether or not bill gates is trustable, well I mean that all depends who you’re asking.
I don’t particularly have any skin in that game.
You’re assertion that the answer will come from pharmaceuticals lacks any room for change.
Yeah , pharmaceutical s are a terrible way to produce medicine. I men why could go wrong? A model based on profit before cure.
So yes, some pharmaceutical might be why gets us out if this mess. You’re not accounting for the fundamental harm in making medicine about profit.
The labour party in the UK had a great idea to nationalise and genericise medicine to cut out the cut throat nature of these corps.
I don’t find the attitude that pharma will get us out of this progressive at all. They’re huge behemoths with a terrible track record.
We need to nationalise health across the world, not let every crises be run by a mafia of corporations.
Look at stem cell research, we should be so much further along. I know it was bush who banned the research on religious grounds, but we know how government work…
I think it’s been bout 20 years since the industry basically moved to Panama. Think we’re we’d be..perhaps cured.
The profit margin should never be part of medicine. It’s only that way cos we allow it.
Well said Conny.
The cognitive dissonance us string in some in here. I question their objectivity.
Ah well. The other stuff is interesting.
I’m not being resold what was quite obviously a heist the first time round
The whole anti Bill Gates thing has distorted more and more over the years.
Here’s a fantastic article on how a group of antiabortionists first misunderstood Gates, that then later led to anti-vaxxers using that misinformation to target him, where they turned the little faux pas of Gates into twisted truth, doctored photos, fake news, to actual outright lies from politicians and money makers who hijacked and further promoted the conspiracy with their own agenda, adding even more rhetoric, that created a mega conspiracy theory.
Even the infamous Alex Jones even got involved in to promote his own anti Gates spin.
It’s worth reading as you can see how this massive rabbit hole all began…
‘The Long, Strange History of Bill Gates Population Control Conspiracy Theories
How the billionaire philanthropist displaced George Soros as the chief bogeyman of the right’
https://www.huffpost.com/entry/bill-gates-coronavirus-vaccine-conspiracy_n_5eb9ab7ac5b69358ef8a9803
Thanks Cort…your blog is extremely well written and very helpful. I got me/cfs from H1N1, and had I had the flu vaccine, I might not have this horrible debilitating, life impediment. I believe in the power of vaccination. Vaccination has saved millions of lives.
I appreciate you continuing to keep us updated on what is going on healthy-wise
Thanks!
You have to remember, not all vaccines are the same. We don’t even know these work properly.
It really doesn’t look like they are to me.
You can be very wary of this rushed vaccine whilst still being glad we have vaccines in this world.
The swine flu vaccine was withdrawn after much less of a signal of harm done to patients.
Also vaccines can Induce long covid.
There are no easy answers. But carrying on in this sane vein is not working. I just wonder how many years it will take for people to realise. I think in America this is mixed with a political leaning. It’s not so much here in the UK although still there a bit.
For me, I’ve had too many medicines hurt me to be ever fine taking this.
Anyways made my point now. God help us all
Thanks for the update and the tip on Paxlovid. I’ll ask my doctor about it next month. I’m always first in line for boosters even though they make me sick for a day or two. nothing long-lasting. Do you know how ME patients are faring when they catch the virus? I’m really worried about it since I’m so close to bedbound already. Long covid on top of pre-existing ME sounds like a nightmare. Thanks for your work 🙂
Cort, thank you so much for your valuable work and thorough research. You’re so incredibly patient with all the comments here – very impressive.
Warm wishes to you!
Im really worried about catching Covid too, as am near bed bound also. Unfortunately for me I can’t risk being vaccinated after the severe and permanent worsening of ME/CFS from just a flu vaccination.
I would like an update on how people with ME/CFS are coping after Covid also, especially the unvaccinated ones like myself. Do we return to baseline or is it yet another drop into a lower level of the baseline.
I cannot get vaccines as I don’t make antibodies. I have had Covid twice. First time in Jan 2020. Second time in March 2020.. First time was like a really bad flu. When diagnosed was immediately put on Clindamycin because have had bacterial pneumonia in past, along with antiviral I take since can’t get flu vaccine and also continued immune supporting supplements I take because of ME/CFS/F. Second time was a little tougher with addition of motor neuropathy. But stayed in bed,took RX and supplements and got through it. Now have diagnose of long Covid, minor symptom of occasional tremors in hand, not painful, just annoying when writing with pen. My MECFS symptoms are the same as before Covid.Absolutely no change,not better, not worse.As long as stay under fatigue level I’m okay. Since I’m retired I can keep from overdoing it. My doctor arranged for me to get monoclonal antibody injection and I have not had any Covid variants although exposed to people who tested positive for Covid. Want to reassure that getting Covid when also dealing with moderate MECFS and F isn’t the end of the world. You can survive it. But one thing I did was when my primary said go to the hospital, I did not. I knew I would be better able to deal with recovering at home doing things that work with the way my body works.
I’m in the UK, and have moderate ME. I had 2 shots of the Astra Zeneca vaccine first 13 weeks apart, followed by a Pfizer booster last November. I was pretty ill after the booster, with side effects lasting for several months, making having ME harder to deal with.
Wednesday 15th June, I caught Covid for the first time (Omicron). On Friday 17th June, paramedics were sent to me to decide if I needed to go into hospital, as I was struggling to breathe. They decided I could remain at home, with the proviso of if I got any worse, my family were to phone for an emergency ambulance (thank you, God, that I live in the UK with the NHS!). I was sleeping 22+ hours/day, breathless, high temperature and cough. Thank God, I’ve recovered, but my ME is now worse, any effort exhausts me – having a shower means I can do nothing else, I’m still not eating properly, and am sleeping 12+ hours at a time. I’m looking forward to my next booster in September, this year.
Shirley, I’m so sorry to hear how bad it was and that it set you back. I watched Jarred Younger’s latest video showing brain problems in ME, and he pointed out various things, but I didn’t know that brain temperature is higher than usual in ME and goes higher during a relapse which is part of what triggers symptoms. I always get a low grade fever during relapses, 99.2 or so, but brain temps are higher than body temps. So I thought I would try to reduce it with full-strength tylenol. I tried it on my last relapse and it was my mildest one so far. Typically relapse symptoms show up in the morning for me, increase over the day, then slowly fade over a week. With the tylenol, the tachycardias and brain fog eased off over the first afternoon instead. That was yesterday. Today I’m tired but no other symptoms, so I’m holding out hope this will continue to help me. I don’t usually have a fever except during relapses. https://www.youtube.com/watch?v=DU0UgWGyi0A
For those that had a problem with an MRNA vaccine, there is another traditionally produced vaccine available in many countries. It is called Novavax. https://www.ama-assn.org/delivering-care/public-health/what-sets-apart-novavax-option-other-covid-19-vaccines
Brendan’s discussion and refs and links above very interesting. Thanks!
Some of you may have heard of “Chronic Fatigue Syndrome”
Not likely though, because no one acts like it.
Perhaps the name, but nothing of the history of this syndrome.
The Holmes CFS definition was coined in 1988 after a strange outbreak in Incline Village Nevada.
A marathon runner who had been in China came back with a flu that wouldn’t quit.
Within a week, the whole town got sick with what Dr Daniel Peterson called “A Chinese flu”
This flu raged from November 1984 until October 1985, then suddenly stopped.
The reasons for this have never been explained or even discussed, as all researchers simply ignore it.
But I can tell you that Dr Peterson believed a “Typhoid Mary” either died or left town. Dr Cheney wasn’t sure, but told me this.
“These types of viruses acquire mutations which can be lost after passing through an immune competent host, which defeats the mutation that made it human transmissible”
Dr Cheney believed that the way this flu moved through the population and suddenly disappeared was consistent with this profile.
Since no one even remembers that CFS started with a “Chinese flu”, this is very compelling that people know absolutely nothing about CFS history, or surely this would have been brought up at some point.
When you don’t believe science then how do you decide what to believe? What is a better source of information than sound scientific method? It’s not perfect certainly and I’m not naively suggesting it doesn’t sometimes get tainted by big money and politics. But if you choose to uniformly disbelief scientific evidence that is objectively presented, you must then believe in things that are on much weaker ground. After reading these posts that seems to be the case.
Science has no conscenscus tho. The whole point if the scientific method is to disprove continualky to sharpen the theory.
This is the problem any discourse has been silenced. Add to that the way pharmaceutical s Syphon up much of the new scientific intake , have paid hundreds of millions to the CDC and continually lobby government and you have a very loaded game. Not recognising the inherent problem here is very naive
It is not believing in science. Science is the best we have. But i don”t believe all scientist, that is a big difference. Especially with the Pfizer study. It is never repeated by indepent scientists. That is the whole problem with corona. There is no time because the virus spreading to fast.
independent researchers who want to investigate excess mortality are not allowed to use more data to establish connections. While and statistically there are very clear links between deaths and prior vaccinations. The data needed to establish a causal relationship is lacking. If there is, then Pfizer and other pro-corona vaccination researchers will of course not benefit at all.
They do everything they can to frustrate or disable other experts. So there is no real transparency as good science should be. If you look at the number of young people and children who died from corona, they are almost 0 or there is a subordinate disease, why still advise this group to get a vaccination? Based on all the data, it is bizarre that the entire world is being vaccinated en masse.
In fact, it’s outrageous and based on fear not rationality. I am for vaccination when there is a serious virus like Ebola . In case of corona, vaccinate people over 60 years old. And anyone who wants it.
But absolutely no mass vaccination. As for the showpiece of bananas and possible side effects is a childish comparison with the data known from systems. When it is summer also people eat more ice cream.
Many people have been vaccinated 3 times or sometimes 4 times within a year with the same drug. This vaccine was tested in December 2020 NEJM Fernando.ea against the original Wuhan corona virus. We are now 2 and a half years further and 5 variants with sub-variants have already emerged. If you look at the flu vaccinations that are adjusted every year and only work for 40 percent. In other words, anyone who still gets a booster against the Wuhan variant should think twice. Continuing to vaccinate chronically with this Pfizer vaccine has never been studied in a double-blind manner. Switching on the immune system 4 times a year and having your own cells make a spike protein as if your cells are a virus is bizarre. The fat globules are found in various organs and cause an inflammatory response, according to research on mice. Assuming that this vaccine has some effect for a few months and you can still pass corona on to your loved ones, it should make people think. And all those so-called millions of people who have been saved, who are they, how old are they, what underlying suffering did they have? Be specific. I am not aware of any double-blind studies. Getting less sick is also a vague concept in an objective sense, which I cannot find in double-blind studies. Be that as it may: another 4 or 5th shot with the same vaccine is dubious for new variants. You’re not going to get a flu shot from 2 years ago, are you?
Well said. Just good common sense. No fear. Fear is the problem here. It’s distorting the issue
Very interesting thread! I wanted to share that I had a moderate reaction to my first vax with Moderna. with the second I used some protocols taking vitamins and antihistamines to lessen reactions, and had NONE! So when the booster was offered I was eager to get it. Used the same protocol, and had what to me was a very severe, yet not anaphylaxis reaction.Two hours after getting the Moderna booster I noticed that my eyes were feeling weird and thought I was reading with the wrong glasses maybe, then noticed queasiness and discomfort, heightened reaction to light, and began to feel very uncomfortable with nausea, would walk (actually lurch) to the bathroom but not able to bring anything up, and then would almost freeze in position leaning against the wall, waiting, seemed like I was in some sort of fugue state. When I did bring up something, the taste was definitely heightened. This went on for 4 hrs. Writing this, doesn’t sound like that bad, but as someone who used to get the flu worse than anyone I ever knew, more frequently and longer, I have spent a lot of time doing self care and feeling crappy, but able to deal with it, and THIS was about my limit. I was just about ready to call 911 or get a friend to drive me to the ER, when I took another antihistamine and the reaction subsided leaving me wrung out and weak. I searched the internet and CDC websites trying to understand the meaning of this for me going forward, regarding any additional boosters and after 2 weeks found a section under adverse reactions on CDC stating that if you get a severe reaction as I did that is not anaphylaxis, but within the first 4 hrs after getting the shot, you should not get any additional shots of the same type. When I spoke to my GP about it, she replied that I had had a strong reaction but that I could get another booster, but I could also wait. Having found out that the 2nd booster does not offer much after 4-6? weeks, and considering that I am very careful, live alone, wear mask when interacting, I decided to forego any mnra boosters. I am excited to hear about the Novavax as a possibility, and even more so , the nasal vaccines!!!! Can anyone give me a perspective on my reaction to that booster…I do not work with an immunologist, or other specialist for my CFS/Fibromyalgia, so just my GP. Thanks and, Best wishes to all, Stay Safe!
Forgot to mention that I realized afterwards that my reaction was the WORST migraine I had ever had. I get the kind that are mostly nausea. thanks again.
I have ME, I cant read loads of anti-vaxer rubbish yet again so I nearly missed your comment, Cort, about brain temperature. Could you extract anything sensible from this so I dont need to try and read dross? I doubt anyone who writes anti vax pages really has ME, although they may get it.
There are some nasal sprays that may be protective against covid https://www.frontiersin.org/articles/10.3389/fviro.2021.746824/full or help if you get it
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7645297/
They need more research but I’ve used xylitol for sinusitis and ear infections so if I buy one and keep handy it wont go to waste. I’ve got a spray with carrageenan in too for use in high risk situations.
Hi Tatt, Thanks for the information. I also found this review paper mentioning the xylitol spray and an additional option, SaNova’s Enova. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8537957/
“4.2. Nasal Delivery of Nitric Oxide (NO)
A treatment developed by the company SaNOtize Research and Development Corp. (Vancouver, Canada) proved to be highly effective and safe in a recently completed clinical trial in the UK [94]. The therapy is also being studied in Phase II clinical trials throughout Canada and in other countries. In the first 24 h, the treatment reduced the average viral load by approximately 95%, followed by more than 99% for the next 48 h. No adverse events were recorded in the trials involving more than 7000 patients testing the self-administered treatment.”
I’m housebound, but my husband is a teacher and goes to the gym a lot, so I’m going to ask him to use it to reduce his chance of infection.
sorry, it’s called Enovid
Enovid was withdrawn from sale, unfortunately. https://www.which.co.uk/news/article/covid-nasal-spray-claims-go-too-far-ajgxS6q6gpYN
Might come back on sale later.
Thanks for that link – I’ll have to read it in stages but looks very interesting.
The second link is interesting. I use a neti pot with Grossan Breathe Ease XL that contains xylitol every single night so I won’t breathe through my mouth with my CPAP mask. I also use it during the day when my allergies are bad. I used to add grapefruit seed extract to the saline/xylitol nasal wash, but stopped years ago. Guess it’s time to add it again.
Have you considered a neti pot? I can’t imagine not using one after all these years. Such a difference in my breathing.
I have a neti pot but havent tried it as since I acquired it I’ve been managing with other things. Currently having hyperbaric oxygen therapy.
Cort, i see hat you’re reading a book about Mrna, maybe you can also listen to Robert Malone. co-researcher of MRNA technology. His advice: no massive Mrna vaccines based on the data they have so far _:)
co-researcher of MRNA technology. His advice: no massive Mrna vaccines based on the data they have so far. Luc Motagnier also warned against massive inetent with the Mrna. There are many scientists who think that way. But if you are critical you will be banned. Even as an expert. Anyone with common sense can imagine that continuing to vaccinate will not be without consequences. You don’t have to be a scientist for that. Time will tell us. Many people I know regret having taken a vaccine with the Mrna. In Germany alone, millions of people with serious side effects and problems have been treated in hospitals after vaccination. This is evident from the figures of insurance companies that have to pay for these treatments. This contradicts all reports that vaccination would cause few problems. This shows that the so-called officially reported side effects are underreported. Objective evidence. I see a lot of people around me with strange health problems, much more than ever. Young people also drop dead more than usual with heart problems, including the elderly. They now call it Sudden Death Syndrome (SDS). How did that happen? Nobody knows officially yet. If I were vaccinated 3, 4 or 5 times with a Mrna vaccine I would be very worried for the future.
“In Germany alone, millions of people with serious side effects and problems have been treated in hospitals after vaccination.”
This statement is false. Germany has about 84 million people, and this would mean at least 3% of the population has been hospitalized because of the vaccine. If that were true, my close friend in Germany would have known, given his wife works as a judge in a major city.
I have lost complete patience with this unhinged anti-vax reasoning. If you don’t want a vaccine, don’t get one. Period. I got the first two Pfizer vaccines last year, and my ME/CFS worsened. But not to the point that I’m bedridden. And that’s key.
Do I regret getting those two vaccines? F^©k no. I’ve had my genome sequenced. Genetically, I’m at high risk for an adverse outcome from coronavirus infection. I also have Alpha-1 Anti-Trypsin Deficiency (A1AD), which puts my lungs at even greater risk for severe damage from COVID, should I survive the infection.
Look, I get it. Iatrogenic disease is real. I have the tetracycline-stained teeth to prove it. But so is death. And that effn antibiotic saved my life when I was an infant, which was the only effective game in town way back when.
What’s the alternative to the vaccines? Get infected and possibly die? Or recover and get Guillain-Barre, which I’ve had? Or live with severe Long-COVID for the rest of your life? The risk for death or GBS or Long-COVID is far less from the vaccine than infection. And having antibodies against spike glycoprotein from the vaccine has been proven to be helpful. This is a no-brainer, at least for me.
Judi i agree that taking this vaccine for people like you and everybody who whant it. And when your older then 60 years. I have been vaccinated for alsmost everything in my life, so i am no anti vax. I have my concerns only about the Mrna technigue and effectivity. I am thinking about taking novavax when adapted to new subtypes myself.
What is the result of their (Paul Erhlich Institute) analysis?
After counting those four ICD codes in their sample, BKK Provita assumes that 216,696 adverse reactions have occurred. They extrapolated that figure to the entire German population for the whole of 2021.
From this, BKK Provita concludes that 2.5 to 3 million people underwent “medical treatment” because of side effects after vaccination. In other words, 4 to 5 percent of the German population would have gone to the doctor because of side effects. Thus, there would be a “significant underreporting of suspected cases of post-vaccination adverse reactions” in the PEI’s official figures.
We now see BA.2 back on stage in the guise of BA.2.75. The variant has therefore been observed in India, but also in the United States, the United Kingdom and Germany.
Scientists working on centaurus point to eight changes compared to BA.2, changes to the ‘spines’ of the coronavirus (the spike protein). These mutations could help centaurus find its way along antibodies. If that’s true, it doesn’t matter if you’ve had covid in the past or have been vaccinated.
Now some good news:
But that does not necessarily have to be a problem, the virologist emphasizes. Although it seems that BA.2.75 spreads faster in India, there is no evidence that centaurus is more pathogenic than variants we have seen before. The WHO does not yet consider centaurus to be a variant of concern.
I wonder why the same people that post anecdotally about negative side effects from the Covid vaccine don’t also write about the tremendous good these vaccines have accomplished in saving lives. Theses vaccines have saved countless lives and yes there are going to be some side effects, the vast majority of which are moderate and end in a day or two. That is why non vaccinated have a higher mortality rate. The problem is if everything in your life becomes one big conspiracy, then the more evidence presented about the efficacy of the vaccine, the more you just think you’re being manipulated by msm, big pharma and the government. Is there a money grab in here? I’m sure to some degree. We’re the vaccines incredibly effective? Yes
You can flip that logic right on its head tho. How many people never reported their injury and therefore the vaccines look safe
Also given the ripe old age many of these people died, a big number of them in care homes here in the ukz how many of thise actually died of covid rather than having covid but dying of old age
You just want to believe there is a saviour out there and all the lies you were fed were correct.
You need to learn from your miscalculation because the whole thing is gonna ramp up again and we will still be having this conversation in two years time.
We can mask up and social distance etc…but no way am I putting anything that new into my body…no chance.
One statement I found in the middle of a CDC document Re. the mrna vaccine: “the long term effects are unknown” I know after my side effects I will never get another one. I have never come down with the vid, just a sore throat for four days. Truly believe vitamin D3 5K IU /day a great help.
I’ve now had four ‘jabs’, three with Pfizer and one with Moderna. I’d do it all over again. I’m highly reactive to all kinds of medications, but with these shots, not much at all–basically just a sore arm. So far, I haven’t had any kind of Covid and I’m almost 70.
I must admit that reading all this commentary has been tedious. I respect peoples various opinions, but also think, ‘Don’t beat up Cort!’ over this. You are entitled to think what you want, but it’s kind of like my opinion on abortion; if you are pro-life, then don’t get an abortion and don’t tell others what to do, but if you are pro-choice, then the decision is up to you.
I always approach ‘science’ with a touch of skepticism, but basically I don’t think they are out to deceive. Perhaps there is some financial motive or a touch of research bias, but it’s up to each individual to do their research–and by that I mean ALL SIDES–and make up their own opinions. And if you must vent, please do it respectfully.
Does anyone know of any disabled groups that are suggesting caution w/ these vaccines, rather than just blindly begging for endless boosters because they’re “immunocompromised”? It’s quite sad how the disabled (including the CFS community) are being portrayed as all the same and in EXTRA need of these experimental drugs.
I anticipate a whole population of disabled who will be made worse after these vaccines. But then will be told, “Well, you surely would have died from Covid if you hadn’t gotten them!” An unprovable, silly claim.
I can almost guarantee Whitney Dafoe didn’t take this vaccine. Agree with you wholeheartedly. It’s getting to the point of incredulity that people are still obsessed with using a Vax that is not working and then shaming those who pointed this out from the beginning.
What the hell is happening? It’s like m.e. people are gaslighting m.e. peopke
OMG! The fear porn in the article.
I have supported Cort for years, but good God, this is a one-sided narrative of doom and gloom that has been spouted for over 2 years. Snap out of it, folks.
Cort, are you accepting money from Big Pharma? This article seems scripted.
Cort, please look into Dr. Robert Malone (RNA vaccine inventor) on Substack.
Steve Kirsch, Dr. Pierre Kory, and Dr. Peter Mccullough for the other side of the story. People need solutions, and vaccines are NOT the solution. Some say (Geert VandenBosch) that vaccination during a pandemic is creating these variants.
There are many early treatments for Covid19 disease.
https://covid19criticalcare.com › covid-19-protocols
https://www.cchfreedom.org/cchf.php/1697/
https://aapsonline.org/CovidPatientTreatmentGuide.pdf
https://covid19.onedaymd.com/
https://aapsonline.org/mccullough-protocol-3-page.pdf
https://www.covidlonghaulers.com/
https://c19early.com/